

Introduction
Certified Registered Nurse Anesthesiologists (CRNAs) have provided anesthesia care to patients since the Civil War.1 Currently, over 56,000 CRNAs practice nationwide and are the primary anesthesia providers in the majority of rural settings and the armed forces.2 Despite this, CRNAs continue to face challenges at the local, state, and national levels, including restricted scope of practice or insurance reimbursement reductions and denials.3 Geographic locations with higher concentrations of physician anesthesiologists may overpower CRNA practice and limit their scope of practice and autonomy through their influence at the institution level as well as in the state and national legislature.3 Historically, physician anesthesiologists have exhibited both robust advocacy and political action committee (PAC) activity compared to CRNAs.3 Some of the issues experienced by the CRNA profession are exacerbated by the fact that many CRNAs either lack exposure, motivation, or political astuteness.4 Political astuteness is defined as political skill and awareness as well as understanding of legislative and policy processes.5
As a group, physician anesthesiologists tend to be more involved in policy-making and advocacy than their CRNA counterparts.6 The American Association of Nurse Anesthesiology (AANA) PAC raised $1,619,488 during 2020 whereas the American Society of Anesthesiologists raised more than double, with $3,891,898 in donations.6 Physician anesthesiologists are also more politically involved at the national level.7 For instance, there are currently a total of 19 physicians in Congress with 15 serving in the House of Representatives and 4 serving in the Senate.7 Of the 19 physicians, one is an anesthesiologist who holds a seat in the House of Representatives.7 Meanwhile, the nursing profession as a whole only has 2 representatives in Congress.8 There is no nurse representation in the Senate, nor is there CRNA representation in either chamber of Congress.8
The imbalance of representation continues at the state level. In Maryland, for example, there are approximately 900 CRNAs but only a small fraction would be considered politically astute with regular involvement in state advocacy and policy advancement for CRNAs.9 These individuals are deeply involved within the state nurse anesthesiology organization as board members, attend political fundraisers, and attend state legislature hearings on important issues relating to the profession.9 Increased CRNA advocacy involvement can be achieved in Maryland as well as other states in the United States.
CRNAs continue to face challenges to their scope of practice. Greenwood and Biddle10 surveyed members of the AANA to investigate scope of practice and how opt-out legislation, and practice location affected their perceptions. The authors found that 35.3% of the 1,163 participants stated they did not believe their current scope of practice adequately reflected their education, experience, and training.10 A literature review on CRNA practice and policy by Vitale and Lyons11 found that CRNAs were restricted and challenged in their practice by physician anesthesiologists through compelling political campaigns and utilization of influence on key legislators. However, a strong presence of professional group resistance against physician anesthesiologist-favorable policies, such as the presence of politically savvy nurse anesthesiologists from state and national organizations, was the most significant factor in policy change for CRNA autonomy.11 This study suggests that CRNAs who have a high knowledge of their practice and the laws governing their scope of practice are in a better position to progress the profession towards more independent practices. Because of these challenges, CRNA must be well-versed in policy to advocate appropriately for the profession.
The goal of this study was to increase CRNA and student registered nurse anesthesiologist (SRNA) knowledge of their practice and the legislation regulating it, to increase their political astuteness, and to encourage and foster interest in future advocacy and policy involvement for CRNA practice agendas. Achievement of this goal will be guided by the development and implementation of a legislative toolkit providing vital information on the legislative process and how to advocate proficiently.
Review of Literature
A review of the literature was executed to identify current research related to legislative toolkits and their efficacy in improving political astuteness levels among CRNAs. The literature was reviewed to determine the importance of policy, current political astuteness among nurses, education on political astuteness for nurses, efficacy of legislative toolkits, barriers to political astuteness and involvement, and strategies to enhance political astuteness and involvement. Most recent literature discussed policy and advocacy education in the educational setting, along the continuum of bachelor to doctoral degree programs. Currently, there is a lack of research specifically exploring political astuteness and interest in political participation within the CRNA and SRNA populations. There is also a lack of research pertaining to toolkits to develop political astuteness.
A national study by VandeWaa et al12 sought to obtain the level of political astuteness and participation amongst registered nurses in relation to the 2018 elections. The Political Astuteness Inventory, a dichotomous measurement tool consisting of “yes” or “no” questions to measure the depth of political astuteness, was used.12 After surveying nurses 2 years prior to the 2018 elections and a month after the elections occurred, the authors found that 20 of the 21 measures in astuteness decreased from 2016 to 2018.12 These measures included voting in the most recent election, supporting their state professional organization’s political arm, actively supporting congressional candidates, and writing letters to legislators about health-related issues.12 Fewer than 50% of nurses in the study knew the names of their state senators or representatives in Washington and fewer than 30% knew at least 2 issues related to the profession that were being discussed at the state or federal government levels.12
There are some similarities to political astuteness levels when comparing registered nurses to advanced practice nurses. Even though political astuteness levels were increased in advanced practice nurses, compared to baccalaureate-educated nurses, political participation in policy and overall level of astuteness remained low.13,14 A study measuring the political astuteness of nursing students after a legislative day used the Political Astuteness Inventory and found that students scored in the lowest category, “totally unaware politically”, before the intervention but improved after the legislative day.13 Using the Efficacy Index, a tool derived from the American National Elections Study and political efficacy theory, a study found a higher political efficacy score amongst nurses with graduate-level education and education in policy, although political efficacy was not officially defined.14 Despite the increase in political astuteness with educational ranking among baccalaureate of science in nursing (BSN) students and CRNAs, there is still an overall lack of collective astuteness and political participation for the nurse anesthesiology profession.12 A study on the impact of professional involvement education on political activism in SRNAs found that policy curriculum requirements such as legislative days can aid in empowering continuous participation in the future.4
There are many barriers to political astuteness and participation among nurses.15,16 Nurse-specific challenges include a lack of motivation and interest in politics, time constraints, a lack of resources, and a lack of mentorship from nurse leaders.15 Doctor of Nursing Practice students were more likely to witness and raise awareness of practice barriers and be more politically active than other types of nursing students.15 A study on experiential advocacy learning via legislative days on Capitol Hill for nursing students suggested that a strong foundation of advocacy and knowledge can lead to a more concrete commitment to legislative and political activities even after graduation.16 The key to involvement is developing well-structured and well-developed learning programs that can mold future nurses as legislative policymakers to influence healthcare policy.16
Increased political astuteness not only gives an individual a sense of empowerment but can have a lasting impact on the profession.12,17 For example, nurses could familiarize themselves with newly introduced state or federal bills and determine which ones can be used to promote positive changes for the profession.12 In an integrated review of challenges, extent of involvement, and impact of involvement in politics for nurses, the authors found empowerment as having the greatest impact on nurses’ involvement in healthcare policy and advocacy.17 Empowerment leads to political involvement which results in political progression.17 These progressions include the development of political nursing organizations at the state and national level and the collaboration of nurses with political leaders in Congress.17
Toolkits have been demonstrated to be an effective interventional source for a researcher’s specific goals.18,19 A literature review evaluating toolkit efficacy as an implementation tool for clinical care found that effective toolkits included high-quality evidence, a rationale for the inclusion of toolkit components based on goals, and guidance on the implementation process.18 Another review on the efficacy of toolkits used to disseminate health information and change healthcare provider behaviors demonstrated that out of the 31 studies evaluating toolkits, 21 of those reported that the toolkit was either useful, satisfactory, or resulted in a change in practice.19
There is minimal existing research on the use of legislative toolkits for CRNAs as an interventional tool.20–22 Njapau-Dove20 created and implemented a policy toolkit for prescriptive authority for CRNAs which included sample letters to policymakers, policy briefs, and information about the CRNA profession. They found that 71.4% of respondents strongly agreed with the necessity of the toolkit and would likely be supported by Maryland CRNAs in promoting prescriptive authority towards legislators.20 Popoola21 developed a policy toolkit for full practice authority in Veteran Affairs hospitals for CRNAs containing emotionally engaging personal stories, elevator speeches, and policy briefs. They found that 83.3% of respondents strongly agreed with this health policy toolkit and believed it would likely be supported by CRNAs in Maryland.21 Sullivan22 explored the development of resources in the form of a toolkit to promote CRNA engagement in policy advocacy at the state level. The toolkit developed to promote CRNA engagement in policy advocacy included information about current political issues for nurse anesthesiologists in that state, a sample letter to a state representative, a state organization fact sheet, and information regarding who CRNAs can contact to increase their political astuteness.22
Toolkit
The CRNA/SRNA Legislative Toolkit designed by the authors included general information on the legislative branch of state governments using Maryland as an example. Pertinent information such as state government structure, total members, legislative bill generation and progression to laws, important events in a yearly session, and committees were presented. The progression of a bill during a legislative session was explained in the toolkit starting from sponsoring a bill to submitting a passed bill to the Governor.
Other components in the toolkit included important committees concerning the nurse anesthesiology profession. The most influential legislators in those committees who handle healthcare-related bills and issues were highlighted. Instructions on how to locate state legislators were created with step-by-step directions from the participant’s state association and AANA websites. The toolkit also contained an elevator speech, information on the state PAC, and an AANA fact sheet on CRNAs to use for legislative purposes. A PowerPoint presentation was developed for the educational session to streamline the dissemination of information on CRNA policy and advocacy from the toolkit.
Methodology
This section presents the methodology that was used to evaluate the following hypotheses: (1) There will be a change in CRNA and SRNA baseline knowledge about state policy with an online educational intervention presenting the legislative toolkit. (2) There will be a change in CRNA and SRNA political astuteness with participation in an online educational intervention presenting the legislative toolkit. (3) There will be a change in CRNA and SRNA interest in participating in future nurse anesthesiology political/policy agendas following an online educational intervention.
Design
Georgetown University (GU) Institutional Review Board issued an exemption via an expedited review due to the benign behavioral interventions involved. After this exemption, the study was implemented as a single cohort, non-randomized design with an educational intervention presented between a pre- and post-intervention test. A CRNA/SRNA Legislative Toolkit was created using resources from the Maryland Association of Nurse Anesthetists, AANA, and Maryland State Legislature.9,23,24 A virtual educational session on the CRNA/SRNA Legislative Toolkit was presented during a lecture series sponsored by Summit Anesthesia Seminars in the spring of 2024. Following consent to participate, baseline levels of CRNA and SRNA political astuteness and comfort with participating in policy agendas were obtained. Then participants engaged in a live, virtual presentation of the CRNA/SRNA Legislative Toolkit. Upon completion of the presentation, a post-test measuring the same variables was obtained. The surveys were delivered in several ways: (1) via a Qualtrics link emailed to all participants following registration, (2) in the chat box when the event went live, and (3) as a QR code displayed on the presentation PowerPoint slides. Prior to and immediately following the presentation of the toolkit, participants were allotted 5-10 minutes to complete the survey.
Sample
The target population was CRNAs and SRNAs in the United States and the sample consisted of a convenience sample of CRNAs and SRNAs who attended a virtual lecture series via Zoom. Summit Anesthesia Seminars marketed the presentation via their website, email, and social media. Participation was completely voluntary and any participant who attended the virtual meeting could opt to open and complete the surveys. Participants were notified of the purpose of the study, requirements for participation, confidentiality measures, and the population being studied. Informed consent was located at the beginning of the surveys and participants were able to stop at any time by logging out. The voluntary nature of participation was emphasized.
A power analysis was conducted using G*Power Version 3.1.9.7 to determine the proper sample size for the study. The power analysis used an effect size of 0.2, an α value of 0.05, and a power of 0.8. The power analysis type was a priori. For a two-tailed, paired t-test, a sample size of 199 participants was desired.
Instrumentation
Demographic information was obtained before participants completed the pre-test Political Astuteness Inventory. Demographic questions included age, years in practice, highest degree obtained, primary practice setting, location of primary practice setting, current state of residence, current status of membership with the AANA, and title.
Further data was obtained utilizing a tool developed by Philip Clark entitled the “Political Astuteness Inventory”. The Political Astuteness Inventory has been used in other studies to assess political astuteness.5,13,25 Primomo conducted 2 studies5,13 using the Political Astuteness Inventory and determined the tool to be reliable. The internal consistency alpha reliability using Cronbach’s alpha for the Political Astuteness Inventory was 0.945 in one study and 0.989 in another, suggesting very strong reliability.5,13 A study on the political astuteness of BSN students following an active learning experience in health policy also used a modified Political Astuteness Inventory and their study determined a strong reliability with a Cronbach’s alpha of 0.84.25
With permission, the original Political Astuteness Inventory was modified for the purposes of this study.5 Each “yes” was counted as 1 point and each “no” was counted as 0 points.5 The “yes” answers were added for a final score.5 A score of 0-9 points was categorized as “totally unaware politically”, a score of 10-19 points was categorized as “slightly aware of the implications of politics for nursing”, a score of 20-29 points was categorized as " shows a beginning political astuteness", and a score of 30-40 points was categorized as “politically astute and an asset to the profession of nursing”.5
A series of 5 survey questions gauging comfort with political involvement in terms of writing legislative letters, attending political fundraisers, making legislative visits, and providing testimony at public hearings was posed to the participants before and after the educational intervention. The likelihood of donating to either the national or state CRNA PAC was also assessed during the pre-test and post-test portions of the survey. The items were rated on a 6-point Likert scale from 1 = Not comfortable at all to 6 = Very comfortable. This section was found immediately after the Political Astuteness Inventory in the survey.
Completing the pre-test served as consent for participation in this study. Participant anonymity was protected by de-identifying the surveys and using unique codes chosen by the participants for pre-test and post-test matching only. Then, the investigator began the presentation on the components of the toolkit. The PowerPoint presentation included information on states’ legislative branches, a walkthrough of finding legislators with an emphasis on key legislators for nurse anesthesiologists in the state, examples of effective state advocacy and ways to advocate, and a discussion regarding the need for high-performing, knowledgeable lobbyists. A step-by-step process illustrating how state bills become law and how bills can be blocked was presented. Also included were the differences between laws and regulations and the state’s relationships with other professional groups such as the state’s anesthesiologist groups and advanced practice nurse groups.
At the end of the educational presentation, participants completed the post-intervention survey. This survey included the same modified Political Astuteness Inventory as well as the same survey questions gauging comfort and likelihood of political involvement. Demographic questions were not included in the post-intervention survey. In order to match responses, participants identified themselves anonymously by creating a unique code for each participant: the first 3 letters of their mother’s maiden name and the last 2 digits of their birth year.
Results
The live virtual educational intervention involved 112 participants with a total of 76 participants who opened the pre-survey and 70 participants completing it. Of the 60 participants who completed the post-survey, 57 could be matched to pre-surveys using unique personal identifiers. One survey was excluded because the participant did not indicate whether they were a CRNA or SRNA. Therefore, the following analyses were based on 56 participants who completed both the pre- and post-surveys. A statistician used Statistical Package for Social Science Version 29 to analyze demographic and political astuteness inventory information. Demographic information included whether the individual was a CRNA or SRNA, age, degree held, AANA membership status, state of residence, and current nurse anesthesiology program attended for current SRNA. Demographic information specific to CRNAs also included years of practice and primary practice setting (see Table 1).
.png)
Most of the participants were SRNAs (n = 48) compared to CRNAs (n = 8), with 1 participant omitting their response (n = 1). This participant was excluded. All 56 participants reported having an active membership with the AANA (n = 56). States of residency varied among participants. Twenty-six percent of participants resided in Washington, DC (n = 15), while 23% and 18% of participants were from Virginia (n = 13) and Maryland (n = 10), respectively. The majority of the SRNAs were from GU (n = 33). Representation from other nurse anesthesiology programs included Charleston Area Medical Center/Marshall University (n = 5) and Fairfield University (n = 8). There were 4 SRNAs who have held a master’s or doctorate outside of the anesthesia profession. Reported years of experience ranged widely within the group of 8 CRNAs. The years of practice ranged from less than 1 (n = 1) to more than 20 years (n = 2). Most CRNAs primarily practiced in an academic medical center (n = 4), while others practiced in a community hospital setting (n = 2) or private practice (n = 2).
For the pre- and post-education surveys, medians and interquartile ranges (IQR) were provided rather than means because the ratings were significantly skewed. Therefore, scores were compared using the Wilcoxon signed ranks test (see Table 2).
Comfort levels on all items increased significantly from pre- to post-education (P < .001). For instance, comfort levels on the pre-test with a 3.0 median score (somewhat uncomfortable) included writing to their legislator concerning CRNA-related issues, attending political fundraisers, making a legislative visit at the state capital, and providing testimony at the state legislature on issues related to CRNAs. Participants reported being neither comfortable nor uncomfortable with donating to the PAC before the educational intervention. After the intervention, post-test scores increased as participants reported a median score of 5 (somewhat likely) on their comfort levels for all 5 aspects of political engagement.
Participants were scored on their level of political astuteness using the modified Political Astuteness Inventory. To determine whether particular areas were more or less affected by the educational intervention, the answers to the individual Political Astuteness Inventory questions were examined and then totaled (see Table 3).
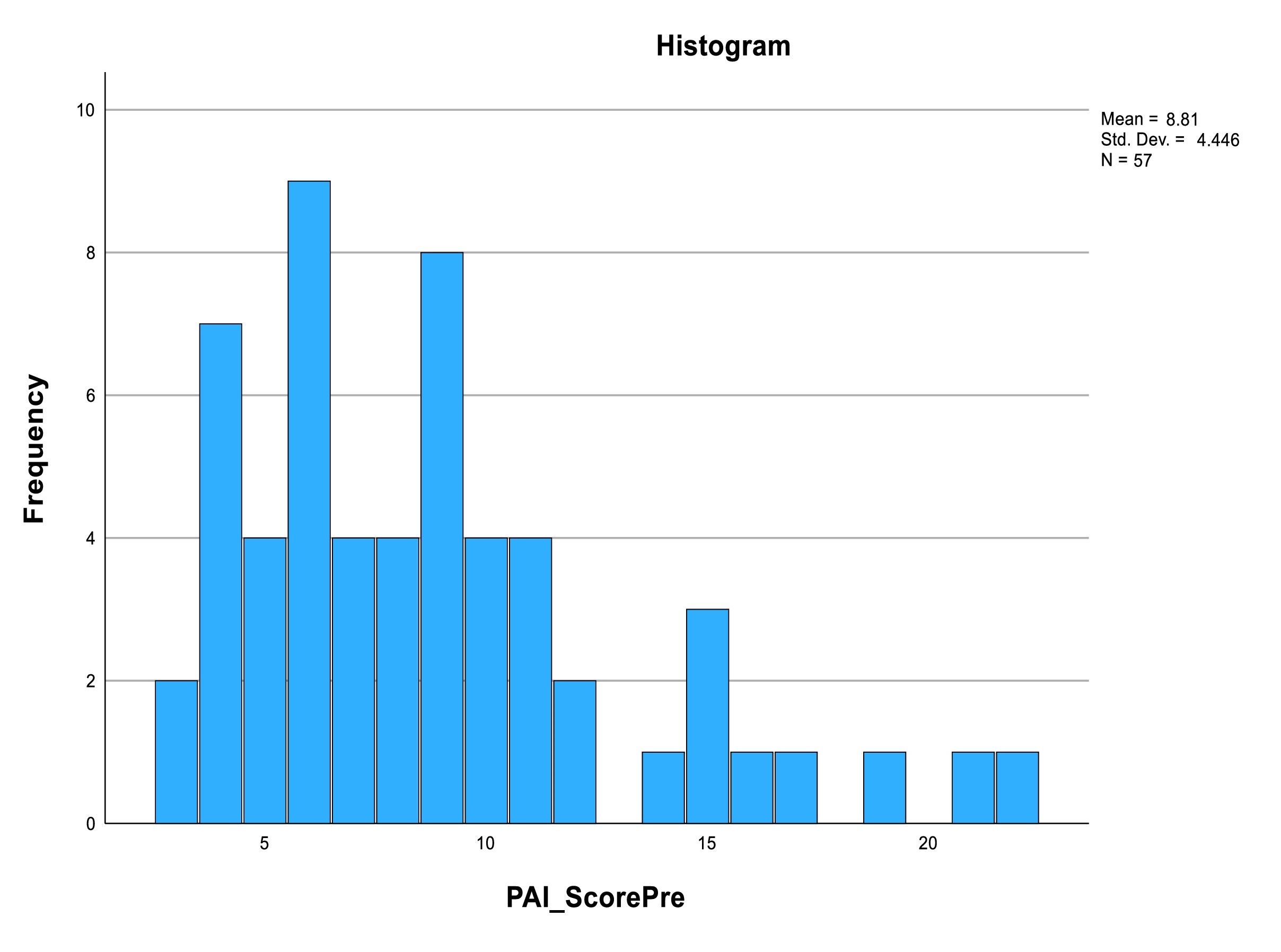
A paired samples t-test was used to compare scores. There was a significant increase (P < .001) in Political Astuteness Inventory score from a mean pre-training of 8.8 (SD = 4.5) to a mean post-training of 13.0 (SD = 4.6) (see Figures 1 and 2).


Pre-scores were somewhat skewed to the right which correlates with previous studies measuring political astuteness on nurses and highlighting the lack of baseline astuteness amongst this population.5,13,22 The post-scores were normally distributed, allowing the use of a parametric t-test instead of nonparametric Wilcoxon signed ranks.
The mean scores increased from a level of “totally unaware politically” on the Political Astuteness Inventory to “slightly aware of the implications of politics for nursing” after the educational intervention.
When comparing Political Astuteness Inventory scores between CRNA and SRNA participants, CRNAs scored slightly higher (M = 10.9, SD = 5.3) than SRNAs (M = 8.5, SD = 4.3) on the pre-test (P = .164). The CRNA mean post-test score was 12.8 (SD = 7.1) and the SRNA mean post-test score was 13.0 (SD = 4.1, P = .870). The SRNAs had a larger gain in their scores (M = 4.6, SD = 4.1) than CRNAs (M = 1.9, SD = 2.6, P = .78). CRNAs and SRNAs rated their comfort with political engagement questions similarly. There were no statistical differences comparing pre-test and post-test Political Astuteness Inventory scores between CRNAs and SRNAs or comparing the difference in scores between the 2 populations. In the pre-test, CRNAs were significantly more likely to say they would donate to the PAC than SRNAs (Mann Whitney, U = 87.5, P = .014).
There were no differences in ratings of comfort with involvement in political processes between GU and non-GU SRNAs on the pre-survey. The Mann-Whitney test was used as the data was skewed. In response to the post-survey question, “How comfortable do you think you will be now with providing testimony for issues related to CRNAs?”, the median rating for non-GU students was 6 (very comfortable) versus 5 (somewhat comfortable) for GU students.
Discussion
This study aimed to close the knowledge gap on the policies and regulations governing CRNA practice, the state legislative process, and the importance of political astuteness and engagement for the profession. This was achieved by implementation of a legislative toolkit. The results suggest that policy educational interventions may improve this political astuteness among CRNAs and SRNAs and improve their comfort with engaging in future policy and advocacy endeavors.
Both CRNAs and SRNAs had a significant increase in their Political Astuteness Inventory scores following the educational intervention, with CRNAs having a higher baseline score. However, the increase in scores for CRNAs suggested that even CRNAs can benefit from an educational intervention on policy and advocacy. The gap in political astuteness between CRNAs and SRNAs before the educational intervention was small (M = 10.9 vs. 8.5) and may be due to growing policy and advocacy education within doctoral nurse anesthesiology programs.
These statistics are similar to the results of other studies that have used the Political Astuteness Inventory to measure the political astuteness of nurses. Byrd et al25 implemented an active learning course on health policy and found a significant increase in political astuteness scores from a pre-test mean of 10 to a post-test mean of 25.7. Primomo5 also found a significant increase in political astuteness levels with the implementation of a health policy course for baccalaureate nursing students. Political astuteness scores rose from a mean of 13.6 before the intervention to a mean of 23.1 after the intervention.5 Multiple studies demonstrate the efficacy of a live, interactive learning course in improving knowledge of policy and advocacy.5,25 Sullivan conducted a similar study specifically exploring the political astuteness of CRNAs.22 Using the Political Astuteness Inventory, mean political astuteness scores increased from 24.8 to 29 after learning activity participation; these results are consistent with other studies using the Political Astuteness Inventory as a measurement tool to study a nursing educational intervention.22 More studies focusing on political astuteness specifically among CRNAs should be conducted to build on these findings.
Active membership in the AANA was one of the most represented methods of participating in advocacy. All 56 participants indicated they held membership in the AANA. This suggests that participants understand the value of being a member of their state and national organizations and are actively paying their dues annually. They may also find value in tracking continuing education credits or using AANA resources for state policy and advocacy. Another well-represented method was being registered to vote; 92.9% of participants (n = 52) marked “Yes” to being registered to vote on the Political Astuteness Inventory. Voter registration is the first step in voting for champions of the nurse anesthesiology profession at the state and federal level, although not all participants who were registered voters actually voted in their last state election. This suggests that providers could benefit from more education on state legislators, including which ones will advocate for the profession.
Only 10.5% (n = 6) of participants indicated they knew who the nursing champions were among members of the United States Congress. After the educational intervention, the number of participants who knew which state and federal legislators were supportive of nursing rose from 6 to 25, a 400% increase. This type of simple improvement in political astuteness can help to advance the profession.
The largest increases in “Yes” responses between the pre- and post-test Political Astuteness Inventory was on knowledge of the difference between laws and regulations regarding CRNA practice (n = 21 pre-test vs. n = 47 post-test), knowing the process by which a bill is introduced in the state legislature (n = 28 pre-test vs. n = 49 post-test), knowledge of which house and senate committees addresses issues relating to healthcare (n = 9 pre-test vs. n = 38 post-test), and knowledge of how to identify and contact their state lobbyist (n = 13 pre-test vs. n = 39 post-test).
There were several limitations to this study. Based on the power analysis at the beginning of this study, 199 participants were required. An email was sent out nationwide to all individuals who follow Summit Anesthesia Seminars but only 112 participants logged in to the virtual session. Of those 112 participants, only 57 participants fully completed both the pre-test and post-test for a response rate of 51%. The inadequate sample size limits the ability to generalize this data to the target population. CRNAs were heavily underrepresented in this study, with only 8 CRNAs participating in the educational intervention. More studies need to be conducted on this issue to improve its generalizability.
Regarding the measurement tool, the Political Astuteness Inventory, some items in the modified Political Astuteness Inventory could not be affected by a one-time educational intervention such as being registered to vote, attending or providing testimony at public hearings, or being professionally acquainted with a senator or representatives. These items remained in the modified Political Astuteness Inventory to limit change to the reliability of the measurement tool. The tool originally targeted nurses, so its modifications towards targeting CRNAs and SRNAs may change its overall reliability despite a Cronbach’s alpha of 0.84 for the modified tool. Also, the post-test was conducted immediately after the presentation, so knowledge decay is not factored into the results. Future studies should account for a longer period between intervention and post-test measurement.
Since the participants were not randomly selected, sampling bias is a limitation in this study. Only those who were attendees of Summit Anesthesia Seminars had the opportunity to learn about the presentation. A convenience sample in this case does increase the risk of bias. Because not every participant from the target population had the ability to participate in this study, this increases the risk of the sample population not adequately representing the target population, thus diminishing the study’s generalizability. Setting inclusion and exclusion criteria and distinctly defining the target population was used to try and minimize bias. Only 18% of participants selected Maryland as their state of residency, so the decrease in applicability to participants in other states could be a confounding variable.
The majority of participants were current doctoral-level SRNAs with policy coursework incorporated into their curriculum and over half of the applicants were below age 30 so this sample was not representative of the target population. Doctoral level education could confound results as the literature has shown that advanced practice nurses have higher levels of political astuteness levels compared to baccalaureate-prepared nurses. This may stem from a more robust curriculum which may include policy and leadership. The age range of the sample makes a difference because most CRNAs are established providers with multiple years of experience in the profession. Since most participants were below 30 years of age and currently enrolled in a nurse anesthesiology program, this hinders the comparability of this sample to the target population.
Conclusion
A significant gap exists in research regarding the political astuteness of CRNAs.22 Policy and advocacy are vital aspects of the CRNA profession.10 Inaction can lead to long-lasting, negative consequences to CRNA practice at the state and federal levels.11 Currently, there is a lack of knowledge and emphasis within the profession on the importance of policy and its processes.12 A need exists to promote continuing healthcare policy education and awareness.23 Evidence suggests that toolkits can be an effective way to increase knowledge of policy and advocacy.5,13,19 Further research is required on ways to improve the political astuteness of CRNAs; future studies should focus not only on the efficacy of toolkits but also on political participation and astuteness within the profession.20–22