INTRODUCTION
The demand for qualified anesthesia providers, particularly Certified Registered Nurse Anesthesiologists (CRNA), continues to exceed the supply. The main drivers of this discrepancy are multifactorial. An aging population with more complex surgical needs together with a backlog of surgical cases following the COVID-19 pandemic has increased demand, while provider burnout related to the same pandemic and retirements have decreased the supply of providers.1–6 The United States (U.S.) Bureau of Labor Statistics projects a 10% increase in demand within the CRNA profession though the year 2033.7 This is the equivalent of 5,200 provider vacancies each year. Growth in the pool of CRNAs is simply not keeping pace with current demand.
Critical to meeting the growing need for anesthesia providers in the U.S. healthcare system is the expansion of hospital partnerships with accredited nurse anesthesia educational programs to provide clinical education. There is already a long lead time for training in the highly specialized nurse anesthesia profession and newer requirements for doctoral degree practice entry further extend the timeline for increasing the supply of new providers. Nurse anesthesia educational programs are searching for ways to increase the size and scope of trainee pipelines in response to this reality. Expansion includes both growth in cohort sizes of existing programs and development of newly accredited educational programs in the U.S. The growing number of resident registered nurse anesthesiologists (RRNA) will result in more graduates and certified providers, meaning that facilities with limited trainee exposure need to consider establishing or expanding clinical site partnerships. This article serves as a case report of how a level-one trauma academic medical center in the mid-Atlantic region expanded existing clinical partnerships and introduced new partnerships to reduce CRNA resource shortages.
BENEFITS AND COSTS OF HOSTING TRAINEES
Research in the CRNA and broader advanced practice registered nursing field demonstrates there are both benefits and costs to hosting trainees at the individual and institutional level. Experienced providers are often motivated to share their accumulated knowledge and experience with enthusiastic learners.8 The presence of trainees can contribute to a culture of professional development.8 Another important benefit is creating a pipeline for recruitment. RRNAs who have trained at a clinical site are more likely to take a position as a CRNA there9—a direct answer to CRNA shortages. A facility gains the opportunity to evaluate the RRNA comprehensively before issuing a contract. This time is essential to determine fit within the culture and may enhance staff retention.10 RRNAs who train extensively at a site and accept a position there may be eligible for an expedited on-boarding and clinical orientation process which reduces overall orientation time and financial expense.10
The costs of adding trainees to a site include staffing resources for orientation, supervision, and administration. For example, program administration at this institution requires dedicated non-clinical time for coordinators to make assignments for the RRNAs, respond to communications from the CRNA programs, and onboard new RRNAs. The coordinators are experienced CRNAs, and these providers are not available for clinical services during administrative hours. Reduced efficiency in clinical operations is inevitable.11 The CRNA precepting an RRNA will be somewhat less efficient given they are offering education during a case in addition to providing anesthesia care. The RRNA is of course not yet as efficient as an experienced provider and extra time is necessary to complete various clinical tasks, seek out clinical resources, or receive reassurance from the experienced provider.
CLINICAL EDUCATION PARTNERSHIPS
As this institution pushed forward with clinical education partnerships 4 key strategic initiatives were developed, which are described here.
Establishing the Role and Value of the RRNA
The requirements for partnership between an accredited nurse anesthesia educational program and a new clinical site are significant. A full treatment is beyond the scope of this manuscript. Most saliently, agreements must delineate the responsibilities and expectations of each party regarding RRNA rotation opportunities to meet clinical site standards as outlined by the Council on Accreditation for Nurse Anesthesia Educational Programs (COA).12 Among the clinical site standards for nurse anesthesia educational programs accredited through the COA is demonstration of adequate clinical resources to meet graduation and accreditation requirements.12 A nurse anesthesiologist or physician anesthesiologist must be appointed as a dedicated clinical coordinator for the site with the varied responsibilities including the management of mutual goals for clinical placement, learning opportunities, procedures for trainee evaluation, and participation in routine clinical site visitations by program faculty.12,13 Meeting these standards for clinical site partnership requires buy-in on the part of the partner institution.
Initially this institution was hesitant to host RRNAs due to unfamiliarity and lack of knowledge. The anesthesia department had minimal, inconsistent exposure to RRNAs and failed to appreciate their robust clinical capabilities within the context of their training. It was difficult for stakeholders to conceptualize the role of the RRNA within a care team model, which at this institution is typically a 1:3 or 1:4 MD to CRNA supervision ratio. To increase the likelihood of successful cultural change, the group had discussions with many stakeholders from various parts of the institution before beginning the process and at various points along the way. These included the anesthesia department chair, CRNA director, the perioperative services administrator, the education coordinators within the CRNA group, the CRNA group, and the day-to-day operations leads termed board runners. The CRNA leadership and education groups set out the goals to have a consistent RRNA presence within the department, offer them a safe learning environment, and to create a recruiting pipeline.
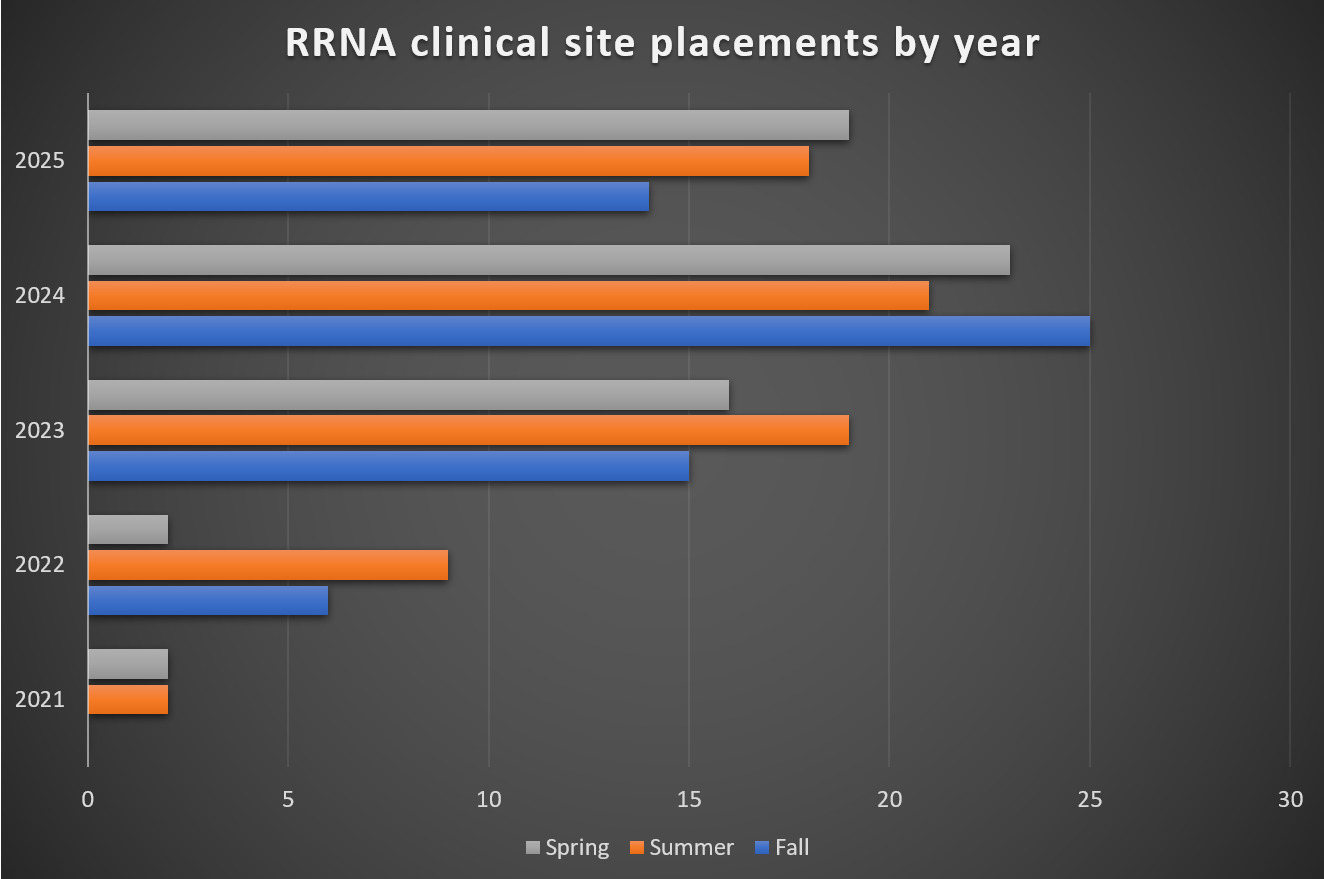
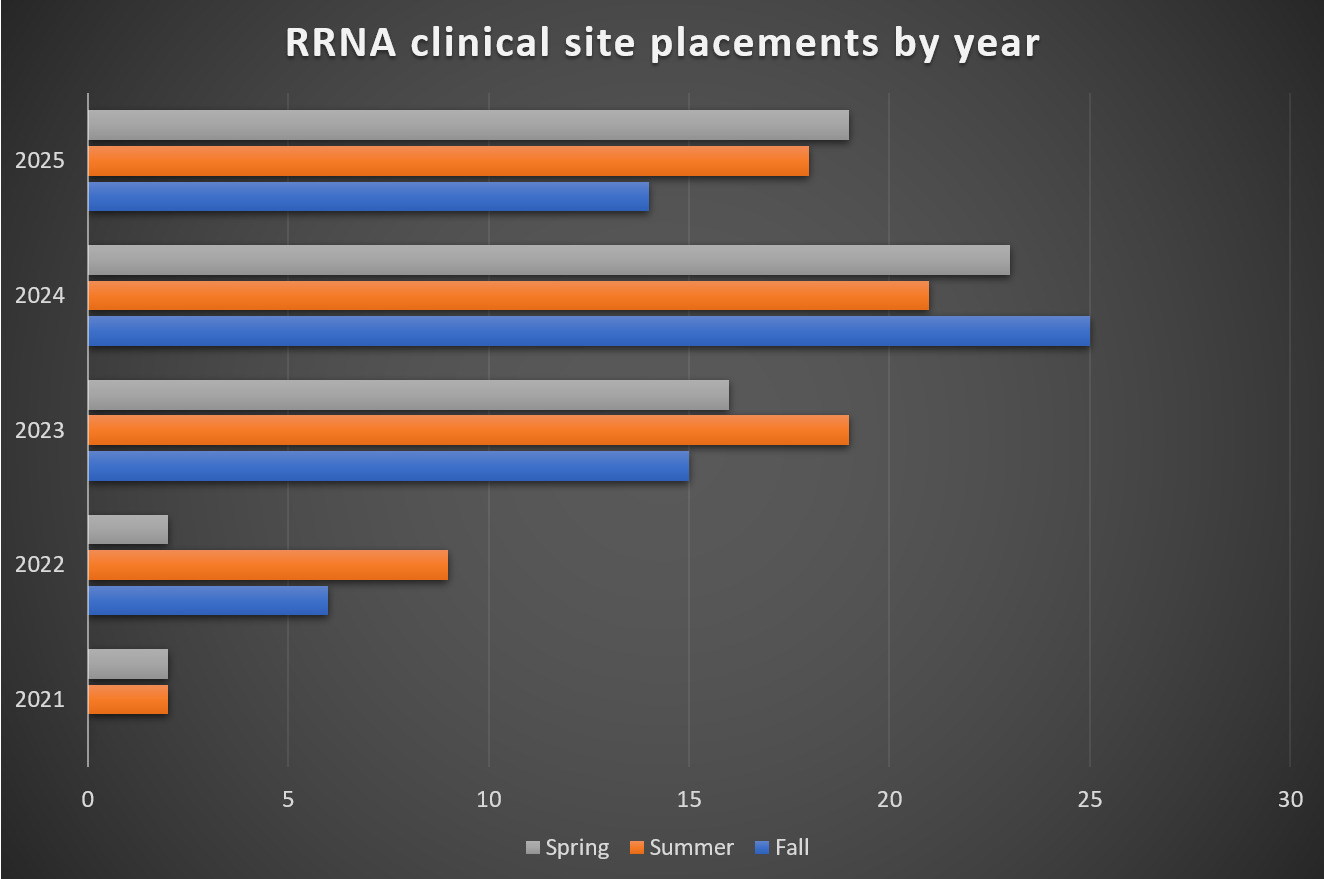
Externally, increased clinical site requests from local programs affirmed the importance of a commitment to training these providers. Internally, the growth of the CRNA workforce expanded capacity for providing clinical education opportunities. Prior to entering the first clinical education partnership in 2014, this academic medical center employed approximately 30 CRNAs. Over the last decade, the CRNA workforce has more than doubled, and a large percentage of CRNAs were willing to take on the role of clinical preceptor. From 2014 to 2020, there was a site agreement with only 1 program, and the site hosted a maximum of 2 senior-level RRNAs. During this time, rotations from this particular program were infrequent. Over the next few years, the site was approached by other local programs to provide clinical opportunities and ultimately signed site agreements with 4 more programs. This led to a gradual increase in the RRNA volume year over year. In 2022, as the department began to feel more comfortable hosting RRNAs, a new program offering primary-site training experiences for junior-level RRNAs was adopted. Growth expanded during this period from an average of 2 per year by 2021, 2 – 8 in 2022, 15 – 19 in 2023, 21 – 25 in 2024, and approximately 14-19 in 2025, comprised of RRNAs from all 5 of the affiliated programs (Figure 1).
As the RRNA numbers increased, constructive feedback was sought out from the stakeholders listed above on the various processes that were implemented, and the program was revised as necessary to grow sustainably. Additionally, RRNAs from accredited nurse anesthesia educational programs are expected to evaluate the quality of their clinical sites and instruction as part of COA Evaluation Standards.12 This feedback is then returned to the clinical site and reflected upon to improve the learning experiences at the site.
Developing Clinical Preceptors and Coordinators to Support RRNAs
With increasing RRNA numbers came requests from CRNA staff for affiliated programs to offer training on best practices for clinical education. CRNA staff at this institution were offered 2 distinct hour-long presentations on clinical preceptorship led by expert faculty from the affiliated programs via zoom. Learning objectives included evaluation of the RRNA as they progressed from novice to advanced beginner, expectations around care plans as they gain more clinical experience, and what to include in daily evaluations. One presentation focused on clinical expectations over time as the RRNAs developed their skills and experience. It methodically reviewed a list of skills, classifying and then reclassifying each skill as independent or requiring varied levels of support throughout the training continuum. The other presentation discussed best practices for appropriate evaluation of RRNAs. Critical to evaluation is delineating processes to fairly evaluate students who are not meeting clinical expectations and providing necessary remediation and support. Discussion also included strategies for offering constructive feedback on care plans, knowledge base, and technical skills. Refining and standardizing CRNA preceptors’ vocabulary for evaluating RRNAs has improved the quality of the feedback RRNAs receive from clinical preceptors. This feedback informs assignments, as detailed later, enhancing RRNA clinical education at this institution.
This program scaled its clinical site coordinators from 1 coordinator to 3 coordinators over a period of 4 years to meet logistical demands. These coordinators are CRNAs who work in close contact with the program site coordinators at the affiliated programs and the local stakeholders within this hospital to ensure a high-quality training experience for the RRNAs. Two coordinators share the responsibility of on-boarding and orienting RRNAs who are new to the site. This consists of arranging access to institutional resources such as electronic health care record keeping systems and required trainings per human resources, as well as a full day of on-site orientation. The third coordinator assists in these tasks as needed, but their primary responsibility is facilitating on-site education ranging from didactic activities to simulation events (detailed later).
This group runs the day-to-day operations of the education program but will confer with the CRNA director on higher level issues, such as RRNA deployment within specialty teams such as pediatrics or obstetrics. All 3 coordinators share the responsibility of making daily clinical assignments for the RRNAs. As this program expanded, the clinical site coordinators created local strategies and guidance around how to effectively deploy RRNAs across the varied clinical sites available at the institution. These include assignments in the main operating room (OR) sites versus non-OR anesthetic locations, acuity of scheduled cases, and various specialty cases. These factors are all matched to optimally align with an RRNA’s clinical experience and required case needs. The coordinators are careful to consider the RRNA’s length of training, prior exposure to specialty cases, and personal report of subjective readiness for complex cases in making assignments.
Clinical coordinators are in frequent communication between anesthesia department and CRNA leadership, operating room schedulers, and board runners. Daily emails are shared among these key players notifying them of which care-team members would be assigned to specific rooms. Anesthesia department clinical faculty are introduced to the specific capabilities of the RRNAs within their assigned rooms. Clinical assignments are thoughtfully made, which accommodates each individual RRNA’s educational needs and interests, while considering their unique level of readiness on the spectrum of RRNA clinical training. Clear communication regarding the presence and capability of RRNAs before and on arrival to rooms is essential and has enabled growth of this program at the institution.
Providing Innovative RRNA Curriculum
Another important component of these efforts to enhance the experience of the RRNAs at this clinical site is dedicated time for lecture and simulation. As previously mentioned, one of the CRNAs in the clinical coordinator role designed an on-site education curriculum. This curriculum balances engaging COA National Certifying Exam content with exploring areas relevant to this clinical setting and the interest and/or expertise of the CRNA staff. Monthly lectures are given most frequently by this clinical site coordinator. However, CRNAs are encouraged to participate, which develops their professional skill of public speaking and deepens their engagement with RRNAs, all while providing important content to the trainees. Topics covered in the lecture curricula thus far include hyperalgesia, processed electroencephalography monitoring, viscoelastic tests of clotting function, processing morbidity and mortality events, journal article discussions, and even retirement planning. Quarterly simulations and workshops, which also include CRNAs, focus on such topics as vascular access placement, use of ultrasound, difficult airway equipment, and the role of the anesthesia provider in code response. Evaluation for these sessions is “teach-back” and successful demonstration of the presented skill.
The RRNA curricula developed at the institution included dedicated time for monthly lecture and quarterly simulations which strengthens knowledge, skill, and professional relationships in the RRNA cohorts. These sessions help the RRNAs to become more knowledgeable about site specific processes or procedures that might be used infrequently. The gatherings also offer an opportunity for RRNAs from the various affiliated programs to interact in a non-clinical setting, to share experiences, and to build camaraderie. The hands-on sessions provide additional opportunities to practice technically challenging skills such as central line placement. The coaching and collaboration evident in the curricula strengthens team dynamics and aligns with the anesthesia department’s overall collegiality goals.
Supporting an Internal Credentialing Pilot Program
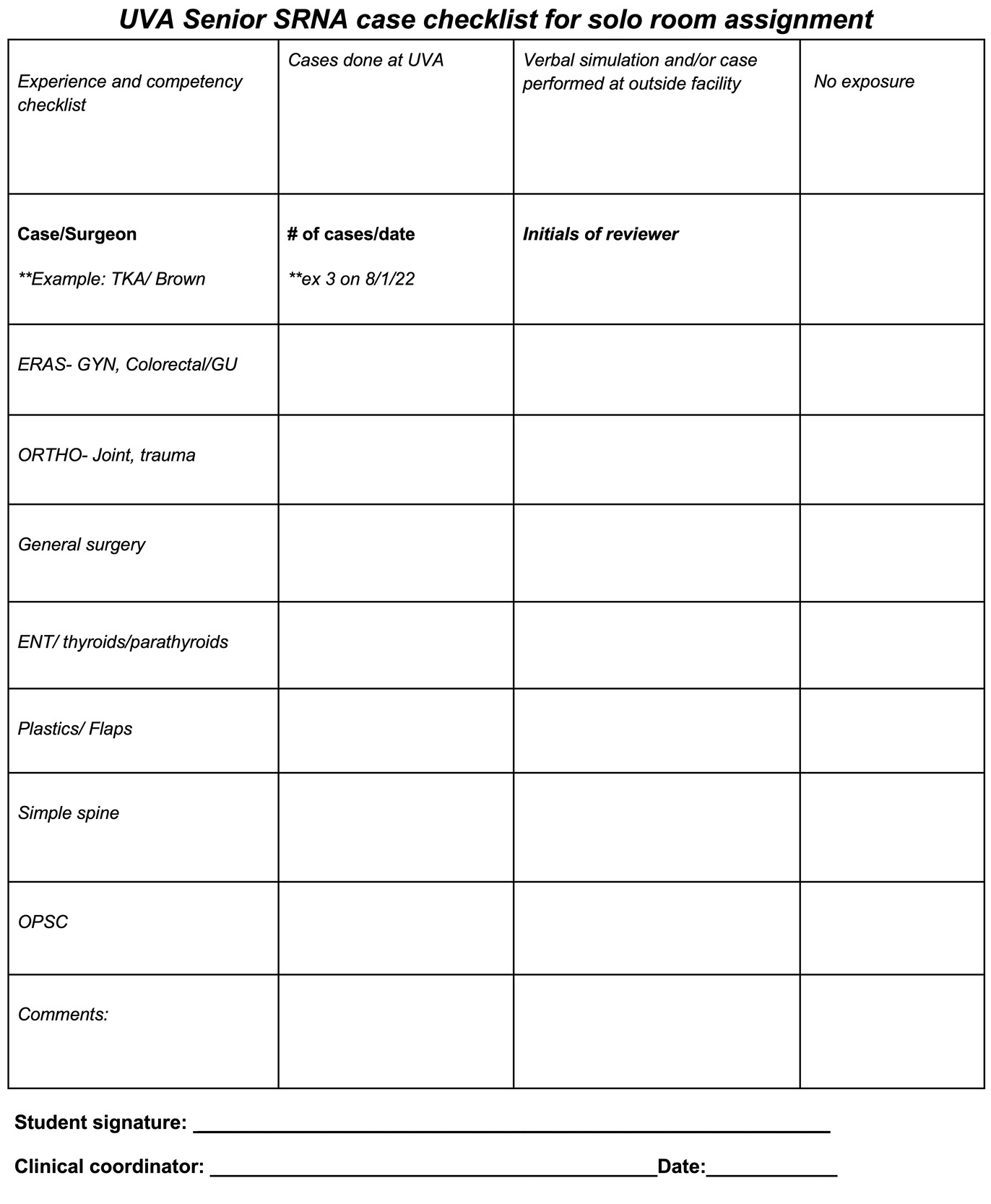
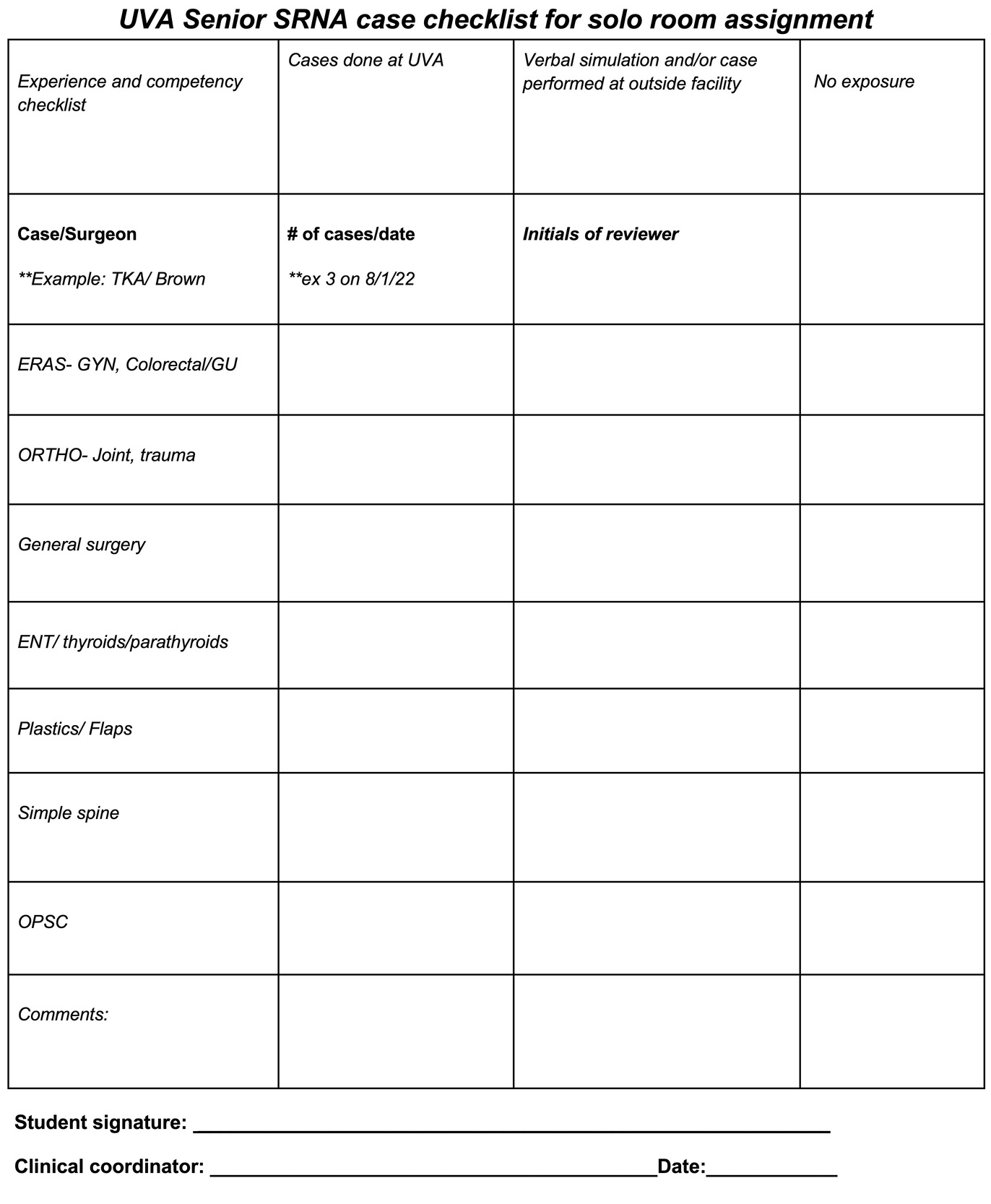
A shift in culture regarding the value of the RRNA, the development of staff CRNAs as preceptors and coordinators to support them, and implementation of a semiformal curricula has steadily increased the presence and reputation of RRNAs in the health system. Key health system leaders signaled their trust and recognition in meaningful ways, and the program has continued to grow. This institutional support allowed the group to develop a novel educational experience for senior-level RRNAs which more closely mimics CRNA practice. Initiated on July 1, 2022, this pilot program mirrors one traditionally used with physician anesthesiology residents by pairing a senior-level RRNA, locally termed solo, with a physician anesthesiologist in a 2:1 supervision model compliant with the COA’s clinical site standards.12 Eligibility for this experience requires what is termed “credentialing.” A solo, credentialed RRNA is (1) in their final year of clinical education, (2) has trained for at least 4 weeks within the health system with no performance concerns, and (3) has successfully completed a procedure and case checklist (Figure 2). The checklist, created by the clinical site coordinators, ensures that solo RRNAs gain the requisite experience with common cases at the institution before being expected to staff those cases without the support of a CRNA. This local process of credentialing is a departmental standard, requiring specific documentation from the anesthesia and perioperative departments to substantiate the eligibility of a RRNA for safe solo practice. The credentialed, solo RRNA is then assigned to physician-supervised anesthesia cases without the presence of a CRNA, just like an anesthesiology resident in the traditional 2:1 supervision model. Research demonstrates that medically directed RRNAs have comparable patient safety records to medically directed CRNAs, MD residents and fellows, thus quality remains similar with this staffing model.14 This novel program has had a modest impact on local staffing resources by increasing the number of available providers and earned positive reviews from the RRNAs who gain an advantage in their transition to practice. A comment from an RRNA from an affiliated program notes “the opportunity to run our own rooms; it exercises both a higher level of critical thinking and also allows us to feel more comfortable in an entry level CRNA role.”
OUTCOMES
The positive effects of the clinical education partnerships within the institution are numerous, including recognition by program sites, enhanced recruitment, a strengthening of culture, and financial impacts. The effort on the front end of this process was more than recouped as the trainees began to positively contribute to the culture of the department and hired within the department as CRNAs.
Stronger Culture
Being a primary clinical site for nurse anesthesia educational programs improves the ability to integrate students into the anesthesia and perioperative departments, benefitting both the trainees and the institution. Primary clinical site RRNAs train at this site for most of their clinical education as opposed to those who opt for elective rotations of approximately 1-2 months. This allows anesthesia providers within the department to become more familiar with the personalities, educational goals, capability and experience of each trainee and over time, for improved enculturation of the trainees into the mission and values of the department.
Clinical precepting has been shown to be a rewarding experience, and the increased opportunities have been well received by departmental CRNAs. In a survey of the CRNA group about their experience precepting, themes that emerged were the reward of observing an RRNAs progression over time, creating a positive learning environment for them and sharing expertise. Another interesting theme was the observation that learning happens in both directions, not just from the preceptor to the preceptee. The group also reported that precepting challenges the CRNAs to stay current in their practice. The group reported that they precept an average of about 30% of their clinical hours. Only 10% felt like they were precepting too much, 47% felt like it was too little, with 43% stating it was the right amount.
Another way the RRNAs contribute to the culture involves clinically focused doctoral practice projects. For the primary clinical site RRNAs, there is an opportunity to identify how their doctoral practice projects can be aligned with departmental and institutional goals to enhance the quality of care provided. Examples of recent projects implemented at this clinical site include a quality improvement initiative for blood product waste reduction, streamlined processes for improved access to nerve blocks for trauma patients with rib fractures, and assistance with the implementation of a peer support program.
Recognition & Recruitment
The RRNAs in one of the partner programs voted this site “Clinical Site of the Year” for 2024 (Figure 3). In a recent summary of RRNA feedback the site received a 96.9% score (n = 20) in the affiliated program’s site evaluation survey (A. Benson, DNP, CRNA, email, July 2025). There is an increased likelihood that RRNAs will seek employment at a facility they have held a clinical rotation with,9 especially if they feel part of a supportive culture, and this recruitment advantage has been observed here. Between 2021 and 2025, 73% of the new-hire CRNAs at this site were new graduates, many from the affiliated programs. Structuring the solo, credentialed RRNA pilot within the clinical education program has given advanced trainees the opportunity to function within a model that more accurately reflects the anesthesia care team they will likely encounter following graduation. These RRNAs will have a better picture of the provider experience at this institution through this opportunity, which may impact their future employment choices upon graduation.
Financial Impact
There has been a positive operational impact through these clinical site partnerships as well. There has been enhanced recruitment from RRNAs that have rotated through this facility, improving the day-to-day staffing outlook, as well as financial benefit from replacing locum CRNAs with the newly licensed CRNAs. Many facilities in the U.S. have been forced into a staffing situation in which the need to maintain surgical case volume during staffing shortages drove the need for locum CRNA resources. At this facility, as many as 21 full-time equivalents of locum CRNAs have been contracted in the last few years and recently this number decreased to 6 which has reduced labor costs by over 8 million dollars per year.
Another financial benefit of hiring newly credentialed RRNAs who have spent significant time training at the institution is a reduction in orientation time from 4 weeks down to 1-2 weeks. An RRNA who has trained at this site as a primary placement has had exposure to all of the main service lines at the institution, including non-OR anesthetic locations, which is the focus of a significant portion of the orientation process, thus the orientation can be abbreviated. During their orientation, a new graduate not familiar with the institution is one-on-one with a seasoned staff CRNA for 4 weeks. For graduates that trained at the institution, that reduction in orientation time produces a cost savings of about $8,000 - $10,000 per hire.
The benefits of the solo, credentialed RRNA under 2:1 physician anesthesiologist supervision has proved to be incredibly positive when evaluating daily resources and the ability to meet the institutional demand for anesthesia services. Staffing flexibility must be considered within the context of the loss of revenue for CRNA services. In the current medical direction model, an operating room with a solo, credentialed RRNA and physician anesthesiologist will be eligible for 50% revenue generation for the physician yet will forego reimbursement for the RRNA under the QK billing modifier—equivalent to a loss of 50% if staffed with a CRNA. However, facility fees charged to patients are often enough to cover the loss of reimbursement for services from a second provider or even the higher labor costs associated with a locum CRNA.
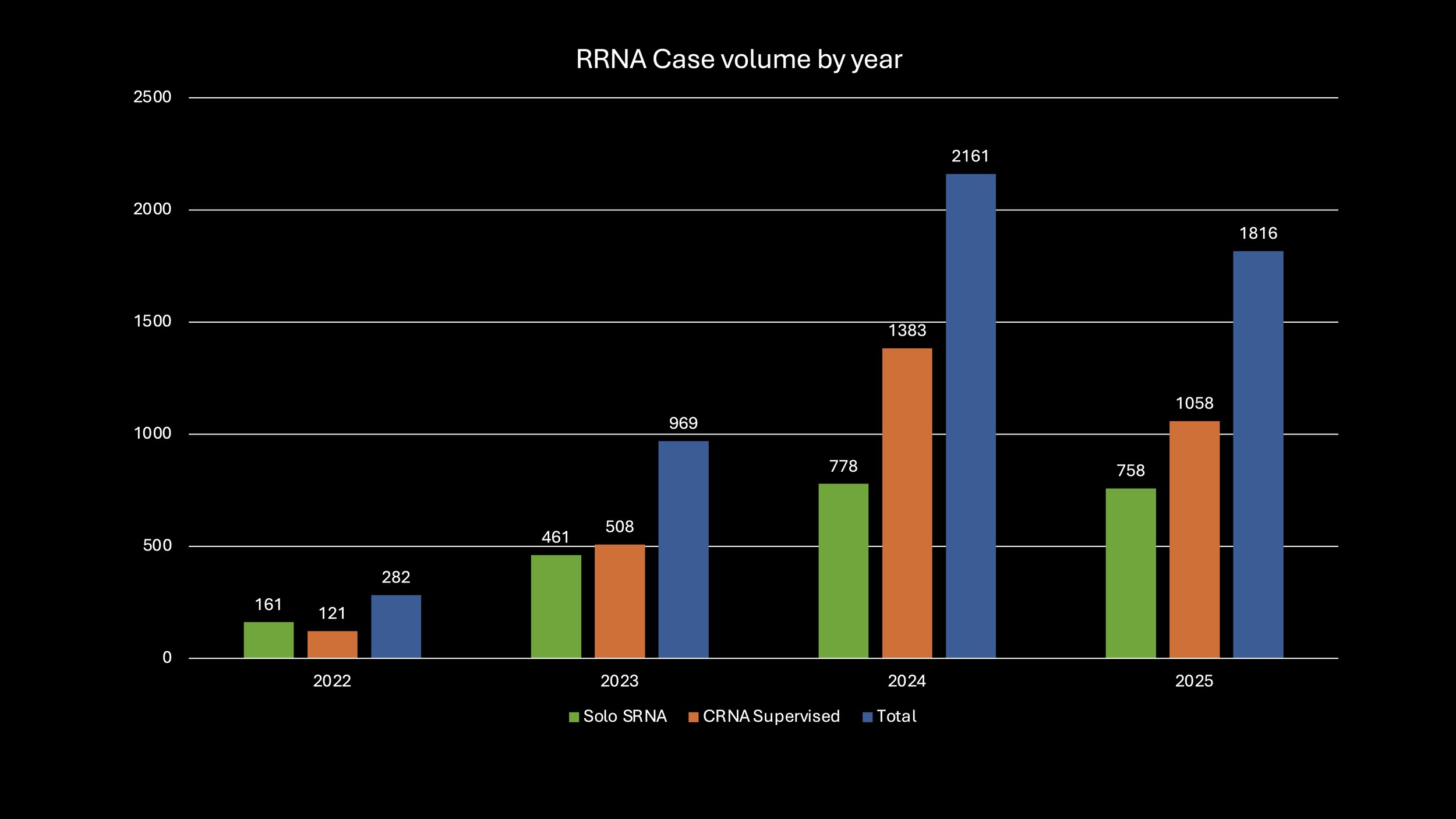
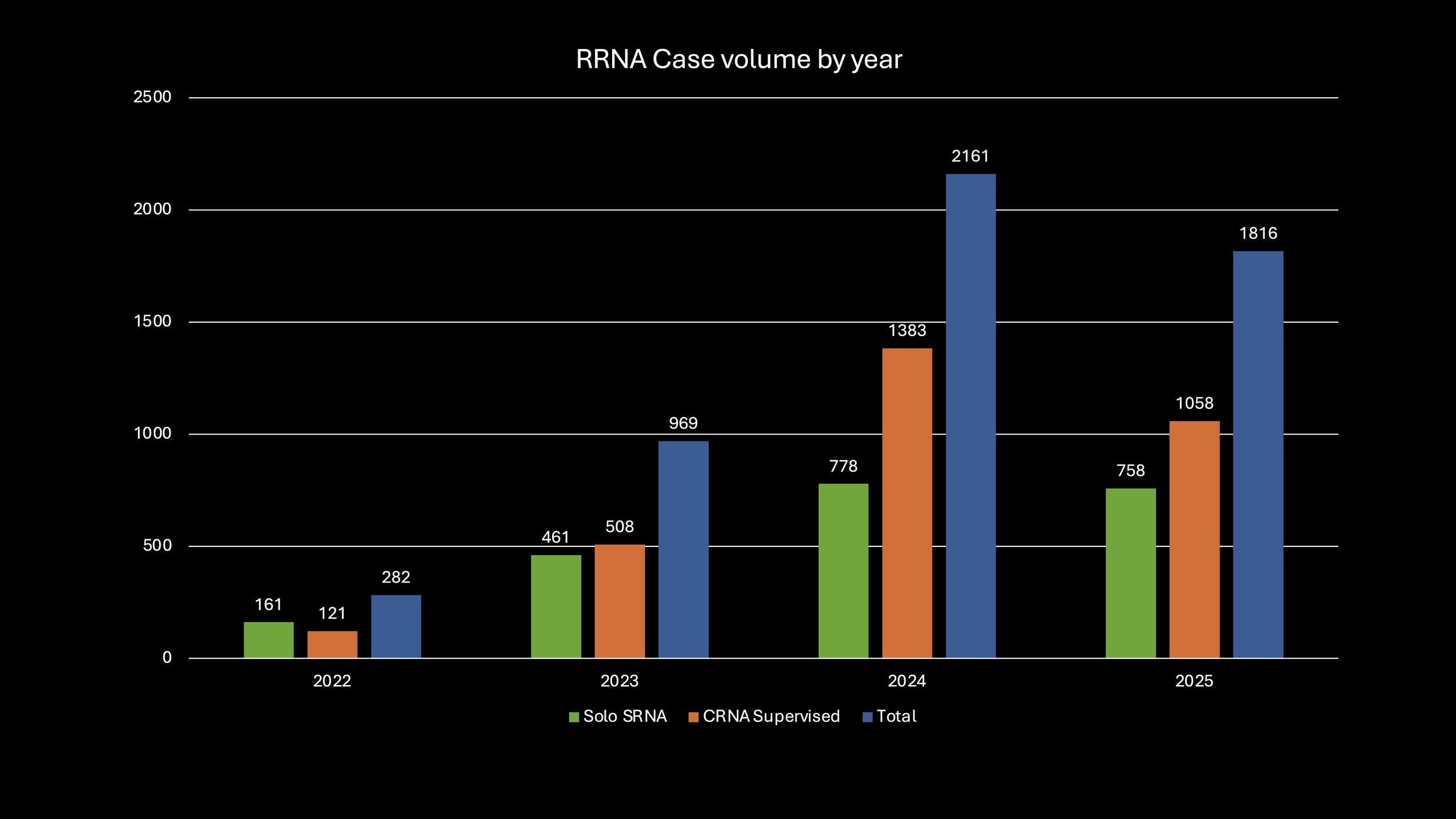
As the RRNA numbers have grown total case volume including their participation has increased as well. Figure 4 displays the annual case volume at this facility by solo RRNA, CRNA supervised RRNA and total volume of cases with RRNAs, starting from 2022 when the cases started being coded in the electronic medical record for RRNAs.
As presented, there are significant financial and staffing benefits to a program such as this, but there are also costs to operating it. Between the 3 clinical coordinators it takes about 8 hours per week to maintain the program, including fielding emails and text messages, making daily clinical assignments, loading the monthly RRNA schedule into the scheduling software, RRNA orientation days, and providing educational or simulation sessions. Some of this time is non-clinical, but a number of these activities often happen during clinical time (e.g. between cases there are a few minutes to make the assignments for the next day). The largest blocks of non-clinical time are the full day of orientation for RRNAs new to the institution and site visits from the programs, but these events are infrequent, happening 4-6 times annually.
DISCUSSION
The intentionally slow and calculated development of this clinical education program allowed the process to be refined in an iterative fashion at a smaller scale while building with sustainability in mind as departmental buy-in increased. These efforts have allowed this institution to support the profession nationally, as well as address long-term staffing needs and reducing labor costs locally. Clinical precepting, an RRNA curricula including lecture and simulation, and the novel solo pilot program have strengthened a culture of education and professionalism in the anesthesia department. A strong reputation as a clinical site has allowed the group to attract top CRNA talent among new graduates.
Regarding sustainability, this site was in a fortunate position to have a high number of CRNAs at a time when there were few RRNAs, creating a large capacity for clinical placements when those requests came. As the program grew, the coordinators tracked how staff were feeling about precepting more frequently and periodically rotated certain staff out of precepting when they reported feeling burned out. There is likely an optimal proportion of RRNAs in any group and determining this is a process of trial and error. While the RRNA numbers vary day-to-day, the average proportion of students in rooms is about 30%. At this point there are discussions to reassess the RRNA numbers to decide if the optimal load might be slightly fewer RRNAs. This is mainly to balance access to complex cases for the RRNAs as well as reducing the burden of precepting for the CRNAs, though the results of the survey suggest preceptor burnout is uncommon.
There is no perfect strategic execution of implementing a program such as this in a large academic medical center, and there were limitations to these efforts. There were bumps in the road along the way, which included various issues such as occasionally navigating personality mismatches with RRNAs and preceptors, implementing and revising corrective procedures for RRNAs that were deviating from expectations, and ensuring that the solo RRNAs were educated on appropriate, timely interprofessional communication with their physician anesthesiologist. Another source of frequent dialog is navigating program requests for specialty cases when within this institution it may not be part of the local culture to have RRNAs in those cases. But through frequent and consistent communication among stakeholders, as described above, this can be navigated relatively smoothly.
In the case of generalizability, success in an endeavor such as this has to do with the specific culture in which it is implemented, and somewhat on the current marketplace for anesthesia professionals. As the CRNA group grew and subsequently supported a larger proportion of the daily anesthesia caseload, and as the CRNA job market tightened up at this institution over the course of the COVID pandemic, it became clearer to local stakeholders that training RRNAs could be an important recruiting tool, and this became an important driver for the success of this program. At institutions where there is strong cultural resistance to novice trainees, there are proportionally fewer CRNAs, or the CRNA group is adequately staffed, motivation may lag and pose a barrier to success. However, the need to establish and grow primary clinical sites for nurse anesthesia educational programs is bigger than any one institution. Health systems must take responsibility to address current and future CRNA workforce shortages through building partnerships with nurse anesthesia educational programs. Such collaborations may prove beneficial to the institution, the services it provides, as well as satisfaction and growth of the provider workforce, which ultimately exerts a positive impact on clinical outcomes and objective financial measures.