Introduction
Emotional readiness has been described as the ability to demonstrate self-awareness, emotional regulation, and resilience in ways that support effective coping during stressful or unpredictable situations.1 In high-acuity, fast-paced clinical environments, a nurse’s level of emotional readiness directly influences decision making, communication, clinical performance, and the ability to provide safe, patient-centered increased situational awareness and reduced susceptibility to cognitive overload, both of which are essential predictors of safe anesthesia practice.2 Despite its importance, emotional readiness is rarely assessed explicitly in nurse anesthesia education, leaving programs to infer readiness only after students enter demanding clinical rotations. Many of the affective competencies required for success, such as stress tolerance, composure, and emotional regulation cannot be evaluated by academic metrics alone.
For admission into nurse anesthesia programs, selection criteria typically include a strong science grade point average, critical care nursing experience, and competitive standardized test scores. However, none of this addresses the emotional readiness of incoming students. As a result, students who excel academically may still struggle to perform clinical tasks under pressure. Although didactic achievement is essential, the ability to maintain emotional stability during complex patient care is equally important. A clear means of conceptualizing and assessing emotional readiness is needed to support student progression and ensure competent future nurse anesthetists. These gaps underscore that emotional readiness remains theoretically underdeveloped, empirically underexplored, and inconsistently supported within anesthesia education.
Theoretically, anesthesia education emphasizes cognitive readiness but pays far less attention to the affective dimensions required for high-stakes clinical learning. The rigor of coursework, management of patients with multiple comorbidities, and mastery of specialized procedures all demand that students not only acquire technical knowledge but also sustain emotional control in rapidly evolving situations. Lakshmi & Lyngdoh3 found that once medical students were trained to handle the emotions of themselves and others, they could achieve success not only academically but also professionally. Yet most nurse anesthesia programs do not formally assess whether students are emotionally prepared for these expectations. This lack of conceptual clarity limits educators’ ability to design curricula, monitor student well-being, and intervene early when affective challenges arise.
Empirically, the literature suggests that emotional readiness may play a distinct role in clinical performance and decision-making among anesthesia trainees, but the concept has not been clearly defined or consistently measured. When students enter the operating room for the first time, they often experience emotions such as intimidation, fear, excitement, and uncertainty. Their ability to recognize and regulate these emotions influences how they interact with the anesthesia team, respond to clinical stressors, and provide safe patient care. Difficulty managing emotional responses can impair communication, clinical judgment, and the learning environment, negatively affecting both patient outcomes and professional relationships.
Clinically, the absence of a well-defined concept contributes to inconsistency in how educators support emotional skill development. Nurse anesthesia students are expected to maintain vigilance, manage complex cognitive tasks, and uphold patient safety at all times. Emotional readiness enhances openness to feedback, supports confidence building, and enables students to apply technical skills under pressure, key components of professional competency. Without conceptual clarity, however, educators lack guidance on how to teach, assess, or remediate this essential dimension of practice.
Emotional intelligence (EI) has a strong positive correlation with emotional readiness, meaning that people with a high level of EI are better prepared to handle challenges and change.4 In their study, Mderis et al.4 noted that when healthcare organizations recognize the importance of developing a strong EI in their nurses, the staff with a high level EI can accept change and adjust more readily. They stated that utilizing strategies like training programs and coaching sessions can develop EI competencies. Also, fostering a strong emotional readiness exhibited a positive attitude towards change in the nurses from the study. Improvement of EI promotes emotional readiness by improving motivation and confidence, stress management, and problem-solving skills, while creating more effective working relationships. There is also a correlation between EI and emotional readiness as seen in academic, career, and organizational readiness. Alternate studies have reported that emotional intelligence positively predicted college students’ learning motivation.5
Although some authors have attempted to define emotional readiness, the concept remains fragmented. Eddinger⁶ described emotional readiness as an individual’s capacity to recognize and regulate affective responses to internal or external stressors, skills that include empathy, communication, maturity, and situational awareness. In nursing, emotional readiness refers specifically to maintaining composure and managing emotional responses while providing safe, compassionate care in high-stress environments.⁷ Yet these definitions vary, lack consistency, and do not fully address the unique demands of anesthesia training.
Because current definitions are limited, inconsistent, and not tailored to the realities of anesthesia education, a concept analysis is needed. Clarifying the defining attributes, antecedents, and consequences of emotional readiness will provide a foundation for developing assessment strategies, guiding curricular design, and strengthening support for students navigating the emotional demands of anesthesia practice. Therefore, the purpose of this paper is to clarify the concept of emotional readiness in nurse anesthesia education using Rodgers’ Evolutionary Method of concept analysis.
Methods
The concept analysis method utilized in this paper is Rodger’s Evolutionary Method, an approach that views the concept as dynamic, context-dependent, and continually shaped by its use over time.6 Rodger’s model is well suited for examining emotional readiness because the concept is not a fixed psychological trait, but rather one that evolves as nurse anesthesia students’ progress through academic training, clinical immersion, and professional development. This method aligns with the understanding that emotional readiness is situationally dependent and influenced by the changing demands of high-stakes anesthesia practice.
Rodger’s Evolutionary Method includes the following analytic steps: (1) identify the concept of interest; (2) identify surrogate terms; (3) identify sample for data collection; (4) identify attributes of the concept; (5) identify antecedents and consequences of the concept; (6) identify related concepts; (7) identify a model case; and (8) conduct interdisciplinary and temporal comparisons. These steps provide a structured framework for tracing how emotional readiness is described across disciplines and for clarifying its essential components within the context of nurse anesthesia education.
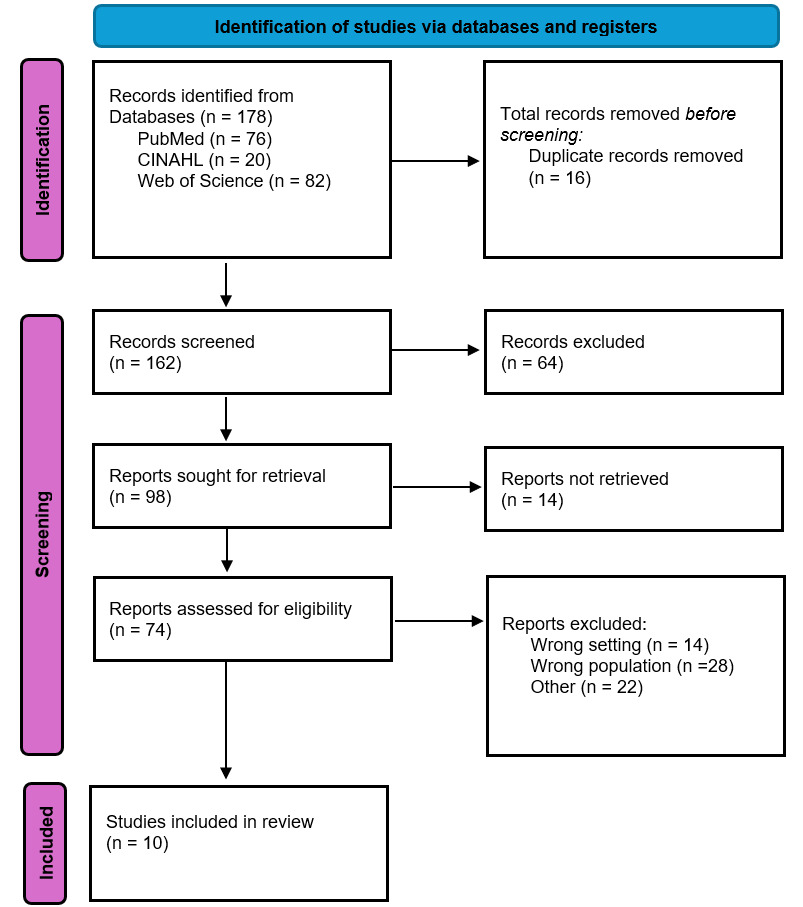
A comprehensive review of literature was performed utilizing PubMed, CINAHL, and Web of Science. The search terms “emotional readiness”, “emotional preparedness”, “emotional regulation”, and “emotional competence” were used. Because emotional readiness is conceptually adjacent to other affective constructs, additional terms (“resilience”, “self-efficacy”, “psychological readiness”, “cognitive ability”, “emotional awareness”, “emotional literacy”), were included to capture broader usage of the concept. Boolean operators AND and OR were used to connect these terms, with population and educational variables “SRNA”, “CRNA”, “APRN”, “student”, “resident”, “education”, and “training” (Figure 1).
The initial search yielded 178 records (PubMed = 76, CINAHL = 20, and Web of Science = 82). All articles were uploaded into EndNote, where 16 duplicates were automatically removed. Manual abstract screening removed an additional 64 records due to wrong setting (n = 14), wrong population (n = 28), and remaining duplicates or non-English articles that EndNote did not detect (n = 22).
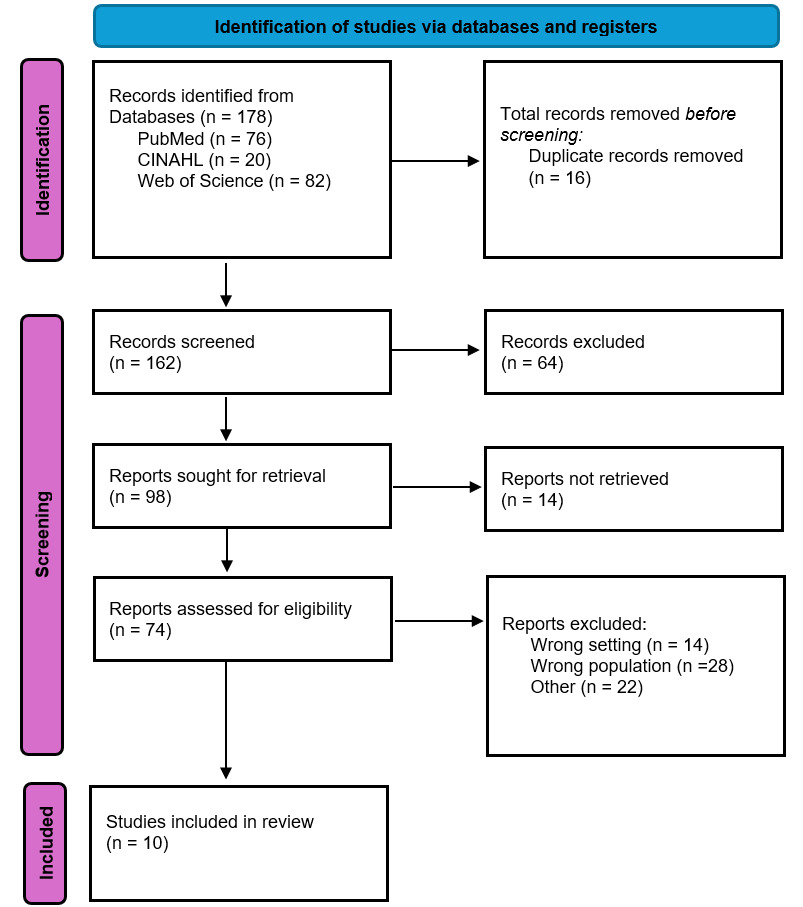
After screening, 98 articles remained for full-text evaluation, only 74 were retrieved for eligibility, and 10 were retained for final analysis based on their relevance to emotional readiness in health professions education (see Figure 1). Articles were included if they (a) addressed emotional readiness or closely related constructs; (b) examined emotional or psychological factors influencing clinical performance; or (c) contributed evidence relevant to defining the attributes, antecedents, or consequences of emotional readiness. Data were organized into an analytic matrix that allowed comparison of definitions, characteristics, antecedents, consequences, and related concepts across studies. This iterative process ensured transparency and supported the inductive identification of conceptual patterns consistent with Rodgers’ Evolutionary Method.
Findings
The analysis of emotional readiness yielded several key elements, including surrogate terms, defining attributes, antecedents, consequences, and related concepts. These findings reflect the dynamic and context-dependent nature of emotional readiness within nurse anesthesia education. The themes presented below emerged from the literature and represent the most frequently described characteristics and contextual influences shaping this concept.
Surrogate terms
Within Rodgers’ Evolutionary Concept Analysis, surrogate terms are understood as alternative labels used interchangeably in the literature to describe the same concept, reflecting the concept’s dynamic and evolving nature over time.6 In the examination of emotional readiness, several surrogate terms emerge across nursing and health professions education literature, most notably readiness for practice, clinical readiness, and psychological readiness. The use of these terms varies by disciplinary context and time period, illustrating the evolving understanding of preparedness in emotionally demanding clinical environments.
Readiness for practice is frequently used to describe a learner’s preparedness to transition from education into professional clinical roles.3,4 Across studies, this term often encompasses emotional components such as confidence and coping capacity. However, emotional elements are typically embedded implicitly within broader measures of preparedness rather than being explicitly conceptualized. As a result, readiness for practice overlaps with emotional readiness but does not consistently foreground emotional regulation and emotional engagement as defining features of the concept.
Similarly, clinical readiness appears in the literature as a multidimensional construct emphasizing the integration of knowledge, technical skills, and professional behaviors required for effective clinical performance.3,5 Emotional preparedness is often acknowledged, particularly in high-acuity or high-stress clinical situations. However, the term is generally operationalized broadly, with limited attention to emotional processes as a distinct focus.
Psychological readiness is another surrogate term identified in the literature, such as studies addressing performance under stress, transition to practice, or adaptation to new professional roles.4,5 This term emphasizes mental preparedness and psychological stability, which intersects with emotional readiness. Psychological readiness prioritizes cognitive appraisal and mental resilience over the dynamic regulation and application of emotions in clinical interactions. This distinguishes it from emotional readiness as an evolving and context-dependent concept. Consistent with Rodgers’ evolutionary perspective, the identification of surrogate terms and related concepts underscores the contextual, temporal, and disciplinary variability of emotional readiness. Clarifying these distinctions supports the ongoing refinement of emotional readiness as a concept and informs its application in nursing education and clinical practice.
Attributes
Attributes are clusters of characteristics that make it possible to identify situations that can be categorized under the concept.6 Based upon the literature, the following attributes demonstrate recurring characteristics of emotional readiness; self-awareness, emotional regulation, resilience and stress tolerance, situational awareness, metacognition, and interpersonal competence (Table 1).
Self-awareness involves recognizing and understanding one’s own emotions and motivations.7 This includes ongoing monitoring of internal state and the ability to identify personal strengths, limitations and needs.8–11 Emotional regulation is defined as the process by which an individual influences which emotions they have, when they experience them, and how they express them.12 Regulation can occur at any point in the emotional process and involves selecting and applying strategies for managing emotional responses appropriately.13–15 It is an ability to modulate anxiety and frustration during high-stakes situations by remaining composed. Within emotional readiness, this attribute reflects the capacity to modulate anxiety and frustration in high-stakes situations while maintaining composure.
Resilience, defined by the American Psychological Association as adapting successfully to adversity, trauma, or tragedy,16 is understood as a learned and developable behavior.17–19 Resilience involves “bouncing back” from difficult experiences and may contribute to personal and professional growth following stress or challenge. Closely related is stress tolerance, the ability to withstand pressure and continue functioning effectively with minimal emotional disruption.20 Together, resilience and stress tolerance support the stability required for emotionally demanding clinical environments.
Situational awareness refers to the perception of environmental elements, the interpretation of their meaning, and the projection of their status in the near future.21 This involves first noticing environmental cues, then forming an accurate understanding, and finally predicting what may occur next.22–27 In healthcare context, situational awareness includes the emotional readiness to rapidly appraise and respond to dynamic clinical situations.
Metacognition is defined as awareness of one’s own cognitive processes and involves deliberate monitoring and control of those processes. Often referred to as “thinking about thinking.”28 Metacognition includes planning approaches, monitoring progress, and evaluating outcomes.29–34 Within emotional readiness, metacognition supports reflective practice by allowing individuals to examine emotional reactions and integrate lessons into future performance.
The final attribute is interpersonal competence, which encompasses personal abilities that influence efficient self-management, communication, and relationship building.35 Interpersonal competence enables individuals to communicate clearly under stress, collaborate effectively, and maintain constructive relationships during challenging interactions.36–40 This capacity is essential for functioning within interdisciplinary teams and executing safe patient care in high-pressure situations.
Antecedents
Antecedents are events, conditions, or phenomena that must occur before the concept can take place.6 In relation to emotional readiness, antecedents identified in the literature are clustered into three categories: individual, educational, and environmental (Table 2). Individual antecedents include a person’s baseline emotional intelligence, coping capacity, personal health status, sleep patterns, and preexisting stress level.40–45 These factors shape an individual’s foundational ability to engage in emotional processing and influence how they respond to emerging clinical demands.
Educational antecedents consist of clinical exposure, structured opportunities to practice coping strategies, simulation experiences involving high-stress scenarios, and facilitated debriefing.46,47 These educational experiences provide opportunities to practice emotional regulation, develop confidence, and integrate feedback – key precursors to emotional readiness.
Environmental antecedents include supportive supervision, mentorship, organizational culture, manageable caseloads, and clear expectations for performance.48–55 A psychologically safe and structured environment is essential for fostering emotional development, enabling learners to engage fully without fear of punitive consequences.
Consequences
Consequences are the outcomes that occur when the concept is present or absent in practical situations.6 In the case of emotional readiness, consequences can be positive or negative, depending on the degree to which the individual possesses this readiness (Table 3). Positive consequences of high emotional readiness include improved clinical performance, enhanced patient safety, and more effective decision-making in stressful situations.56–60 Student novice providers who demonstrate emotional readiness tend to exhibit fewer clinical errors, communicate more clearly, and adapt more quickly to the demands of the clinical environment. Additional positive outcomes include accelerated professional socialization, more efficient learning, and stronger teamwork within the operating room or other high-acuity settings.
Negative consequences arise when emotional readiness is limited or lacking. Lower levels may manifest as increased anxiety, impaired clinical performance during crises, and avoidance behaviors that reduce exposure to critical learning experiences.61–65 These patterns can contribute to missed educational opportunities, higher attrition rates, increased sick leave, and overall reduced confidence in clinical abilities. Collectively, these consequences highlight the essential role of emotional readiness in supporting safe, competent, and resilient practice.
Discussion
This evolutionary concept analysis reveals emotional readiness as a dynamic, multidimensional construct shaped by the interaction of defining attributes, antecedent conditions, and observed consequences within the context of nurse anesthesia education and practice. Rather than functioning as a singular skill or trait, emotional readiness emerges through the convergence of emotional awareness, regulation, adaptability, and reflective capacity. These collectively enable students to engage effectively in high-stakes clinical environments. The synthesis of these components underscores emotional readiness as an evolving state of preparedness that develops over time and varies according to contextual demands.
The defining attributes identified in this analysis, emotional awareness, emotional regulation, adaptive coping, and reflective capacity, do not operate independently. Emotional awareness enables individuals to recognize internal emotional responses during clinical encounters, while emotional regulation allows those responses to be modulated in ways that support safe and effective performance. Adaptive coping facilitates flexible responses to stressors and uncertainty, and reflective capacity supports learning from emotionally charged experiences. These attributes collectively interact to support emotional readiness as a functional state that allows nurse anesthesia students to maintain cognitive clarity, professional judgment, and interpersonal effectiveness under pressure. The absence or underdevelopment of any one attribute may compromise the individual’s overall emotional readiness, reinforcing the interdependent nature of the construct.
Antecedents such as prior clinical exposure, educational preparation, mentorship, and supportive learning environments influence the development of these attributes. High-fidelity simulation, structured debriefing, and progressive exposure to complex clinical situations appear to facilitate emotional awareness and regulation, while mentorship and feedback contribute to reflective capacity and adaptive coping. Conversely, environments characterized by excessive workload, limited feedback, or punitive cultures may inhibit the development of emotional readiness despite strong cognitive or technical preparation. These findings suggest that emotional readiness is not solely an individual characteristic but is co-constructed through educational and clinical contexts.
The consequences associated with emotional readiness further illuminate its significance as a distinct concept. Across the literature, emotional readiness is associated with improved clinical performance, enhanced situational awareness, effective communication within interprofessional teams and safer patient care. For nurse anesthesia students, emotional readiness supports the ability to respond appropriately during critical events, manage emotional stressors inherent to anesthesia practice, and engage in professional role socialization. These outcomes reinforce emotional readiness as a critical contributor to both patient safety and provider well-being.
Consistent with Rodgers’ evolutionary perspective, emotional readiness demonstrates contextual and temporal variability. The expression of emotional readiness may differ across stages of nurse anesthesia education, with early learners focusing on emotional awareness and basic regulation, while advanced students demonstrate greater adaptability and reflective integration during complex clinical situations. Similarly, emotional readiness may manifest differently across clinical environments, such as routine surgical cases versus high-acuity or crisis situations. Over time, repeated exposure to emotionally demanding experiences may further refine emotional readiness, highlighting its developmental and situational nature.
Although related constructs such as emotional intelligence, resilience, and self-efficacy share conceptual overlap, they remain distinct. Emotional intelligence represents a broader capacity to perceive and manage emotions, often conceptualized as a relatively stable ability, whereas emotional readiness reflects a situational state of preparedness that draws upon, but is not equivalent to, emotional intelligence. Resilience describes the ability to recover following adversity, while emotional readiness emphasizes preparedness prior to and during emotionally demanding clinical encounters. These distinctions reinforce emotional readiness as a unique construct focused on in-the-moment emotional functioning within specific professional contexts.
This analysis underscores the need for continued refinement of emotional readiness as a concept. Variability in terminology, measurement approaches, and contextual emphasis across studies suggests that emotional readiness remains an evolving construct. Future research should aim to further operationalize emotional readiness in ways that reflect its multidimensional and developmental nature, examine how educational and organizational interventions shape its attributes over time, and explore its relationship to clinical performance, patient safety, and provider well-being. Ongoing empirical and theoretical work will be essential to advancing emotional readiness as a meaningful and actionable concept within nurse anesthesia education and advanced nursing practice.
Implications for Nursing Practice, Education, and Research
The findings of this concept analysis highlight that emotional readiness has important implications for advanced nursing practice, education, and research. In clinical settings, emotional readiness supports safer decision-making, stronger situational awareness, and adaptability during high-stress events, competencies essential for nurse anesthesia providers. Enhancing emotional regulation, resilience, and interpersonal competence may strengthen team functioning and contribute to improved patient safety.
Within nurse anesthesia education, the analysis indicates a need for intentional curricular approaches that develop students’ emotional readiness alongside cognitive and technical skills. Strategies such as simulation-based stress exposure, emotional intelligence training, guided reflection, and structured debriefing may help students manage clinical uncertainty and regulate emotional responses. Faculty development is also important to ensure instructors can effectively support students’ affective learning needs.
Further research is needed to refine and operationalize the concept, develop valid assessment tools, and evaluate educational interventions aimed at strengthening emotional readiness. Longitudinal studies examining changes across training and research exploring relationships with retention, clinical performance, and patient outcomes will help establish emotional readiness as a measurable and teachable component of advanced practice nursing education.
Programmatic Implications
The findings of this concept analysis have direct implications for how nurse anesthesia programs can operationalize emotional readiness across the educational continuum, from admissions through curriculum design to faculty development.
Assessment during admissions. Emotional readiness should be considered as a complementary criterion during the admissions process, alongside traditional academic metrics. The Emotional Intelligence Test (EMI-T) has demonstrated validity in healthcare student selection, with psychometric properties supporting its use for identifying students with abilities required to succeed in emotionally demanding clinical environments.66 Emotional intelligence assessment tools, such as the Emotional Quotient Inventory (EQ-i) or the EMI-T have demonstrated validity in predicting nursing student success, particularly in domains of stress tolerance and interpersonal capacity.15,66,67 Programs may consider incorporating structured behavioral interviews or situational judgment assessments that evaluate candidates’ self-awareness, stress management strategies, and responses to emotionally challenging clinical scenarios.14,15 Such assessments would not replace existing criteria but rather provide a more comprehensive evaluation of applicants’ readiness for the affective demands of anesthesia practice. Importantly, baseline emotional readiness data collected during admissions can inform individualized student support throughout the program.13,15
Curricular integration. Nurse anesthesia curricula should intentionally incorporate evidence-based strategies to develop emotional readiness alongside cognitive and technical competencies. A systematic review of 19 studies found that simulation was the most effective pedagogical strategy, improving emotional competence, compassion, self-awareness, self-efficacy, critical thinking, clinical practice skills, and teamwork skills.68 High-fidelity simulation with structured debriefing has proven particularly effective for developing situational awareness, emotional regulation under pressure, and metacognitive skills.22,25,27,69 Simulation scenarios should progressively increase in emotional intensity, allowing students to practice affective responses in psychologically safe environments before encountering similar situations in clinical practice.22,23,27,70
Mindfulness-based interventions and reflective practice activities have demonstrated significant reductions in stress and improvements in emotional well-being among healthcare students.1,32,71 Integrating reflective practice and mindfulness exercises into nursing curricula has demonstrated statistically significant increases in both emotional intelligence and mindful attention awareness.72 These can be integrated as brief, longitudinal modules throughout the didactic curriculum. Reflective practice activities, including guided journaling, portfolio development, and contemplative exercises, support the development of self-awareness and metacognition, core attributes of emotional readiness.7,32,34
Programs should also consider incorporating emotional intelligence training workshops that explicitly teach emotion recognition, regulation strategies, empathy development, and interpersonal communication skills.25,32,33,73 A meta-analysis of 23 studies demonstrated that emotional intelligence training significantly improved emotional intelligence (SMD = 1.76), reduced stress (SMD = -1.51), and enhanced communication skills (SMD = 2.72) among nurses and nursing students.73 Combining multiple pedagogical approaches, such as didactic content on emotional competence, role-playing exercises, and real-world application through clinical experiences, appears most effective.25,33
Faculty development. Educators require specific preparation to effectively assess and support students’ emotional readiness. Faculty development initiatives should focus on: (1) recognizing signs of emotional distress or inadequate emotional regulation in students; (2) facilitating effective debriefing that addresses both cognitive and affective learning; (3) providing constructive feedback on emotional competencies; and (4) creating psychologically safe learning environments that encourage vulnerability and growth.31,32,74
Faculty unanimously agree that emotional intelligence skills are essential components of undergraduate nursing curriculum and crucial to cultivating a healthy academic environment, yet require systems-level support for consistent implementation.74 Faculty mentorship plays a critical role in modeling emotional competence and supporting students through emotionally challenging experiences.48–51 Training faculty in trauma-informed pedagogy and reflective supervision techniques can enhance their capacity to guide students’ affective development while maintaining appropriate boundaries.31,32 Additionally, faculty should be equipped to identify when students require referral to professional mental health resources, recognizing that educational support differs from clinical intervention.
Ongoing assessment and support. Programs should implement longitudinal assessment of emotional readiness throughout training, recognizing its developmental and context-dependent nature. This might include periodic self-assessment using validated emotional intelligence measures, faculty evaluation of students’ emotional regulation during clinical experiences, and structured reflection on emotionally challenging cases.14,15,32 Early identification of students struggling with emotional readiness allows for timely intervention, which may include additional mentorship, counseling referrals, or modified clinical progression. Creating an organizational culture that values emotional readiness as essential to professional competence, rather than viewing it as a personal weakness, is fundamental to successful implementation.52–55 This requires institutional commitment, adequate resources, and integration of emotional readiness development into program outcomes and accreditation standards.
Limitations
This concept analysis has several limitations. First, the body of literature on emotional readiness among nurse anesthesia students is limited, with much of the evidence derived from related fields such as medicine, psychology, or general nursing. This restricts the direct applicability of findings to the nurse anesthesia context. Second, because Rodgers’ Evolutionary Method emphasizes context and acknowledges that concepts change over time, the definition of emotional readiness generated here is inherently provisional and may shift as educational and clinical expectations evolve. Third, this analysis is dependent on the available literature and may be influenced by publication bias, particularly studies emphasizing positive dimensions of emotional and cognitive performance. Finally, emotional readiness is a subjective and multifaceted construct shaped by individual, cultural, and environmental factors; therefore, its attributes, antecedents, and consequences may vary across learners, institutions, and practice settings.
Conclusions
This concept analysis demonstrates that emotional readiness is a vital yet often underdeveloped component of nurse anesthesia education. The defining attributes of self-awareness, emotional regulation, resilience, situational awareness, metacognition, and interpersonal competence collectively form the foundation for safe, adaptive, and competent clinical practice. By identifying antecedents, attributes, and consequences of emotional readiness, this analysis provides educators and researchers with a clearer framework to guide assessment strategies and curriculum design. Strengthening conceptual clarity has the potential to improve student performance, patient safety, and continued advancement of anesthesia nursing. As educational programs maintain high expectations for cognitive and technical mastery, intentionally recognizing and fostering emotional readiness will remain essential for preparing resilient and effective advanced practice nurses.