Introduction
Applying what we learn as anesthesia providers is consistently emphasized in the literature as requiring active learning strategies that move beyond passive knowledge acquisition. Active learning supports student engagement and performance,1 promotes deeper conceptual understanding,2 and enhances learning outcomes when compared with traditional teaching methods.3 By shifting classroom time toward application and discussion, active learning increases the value of in-person instruction, supports adult learning principles, and allows clinician educators to connect theoretical content to real world anesthesia practice.
The challenge of the traditional lecture-based learning is the placement of the teacher rather than student in the center of learning.4 As a result, student learning becomes passive with minimal interaction with the didactic content. Conversely, the flipped classroom (FC), also known as reversed classroom, learning model embraces the concept of student-centered teaching that promotes the student to learn through interaction rather than a passive transfer of knowledge from the teacher onto the student.4 To achieve this, the instructor in the FC model distributes pre-class material followed by in-class interaction to promote active learning with the clinical expert. This student-focused model becomes significant considering the high stakes in anesthesiology training, where clinical connection and application of the retained knowledge directly impact the quality of patient care.5,6 In a recent meta-analysis that further supports its practical relevance, the FC demonstrated improvement in theoretical knowledge and skill scores compared to traditional teaching methods.7,8
To help bridge the gap between FC theory and practical application in 2026, this article aims to identify key characteristics of effective FC strategies in the literature and reflect on their implementation within a graduate nurse anesthesia program in the Midwestern United States. Particular attention is given to the unique challenges faced by clinician educators transitioning into academia, as successful implementation of the FC model requires a substantial upfront investment of time and preparation. Faculty must remain ahead in the development of high-quality recorded lectures while simultaneously designing meaningful in-person learning activities that promote discussion, clinical reasoning, and application of knowledge. Although this process requires considerable effort, the investment may be rewarded through enhanced student engagement, greater instructional efficiency, and positive learner feedback regarding the value of active learning and clinically relevant classroom experiences.
Background and Supporting Evidence
This article draws on a comprehensive synthesis of the literature examining the FC model, incorporating evidence from systematic reviews, randomized controlled trials, qualitative surveys, and program evaluations. The analysis centers on findings most relevant to optimizing FC methodologies in anesthesia education and is organized around 5 core themes: instructional design features, student engagement, academic performance, technology integration, and factors influencing successful implementation.
The first core theme is the instructional design features. These refer to the structural strategies used to plan and deliver FC content in a way that promotes active learning. This includes how material is sequenced, the format and length of pre-class content, and the integration of in-class application activities such as case study discussions. Research identified pre-class video lectures combined with interactive, case-based, or problem-solving in-class activities as their core design elements.9,10 Studies also described utilizing blended learning (which is an instructional approach that combines face-to-face teaching with online or technology-enhanced learning activities, intentionally integrating both to enhance flexibility, engagement, and depth of learning) and team-based learning (structures in-class problem-solving in teams) to enhance active participation.11,12
The body of research highlighted that goal-oriented and objective teaching methods, when combined with the FC approach, were effective in structuring learning and improving both training outcomes and teaching satisfaction in anesthesia education.13 Others also emphasized the importance of aligning the FC design with adult learning theories and learner characteristics.14,15 Adult learning theories emphasize self-direction, relevance to real-world experiences, and the need for learners to actively construct meaning through reflection and application. Key learner characteristics include a preference for autonomy, a readiness to learn content that applies directly to professional roles, and a motivation driven by internal goals rather than external rewards. These principles align closely with active learning strategies commonly incorporated within FC models, including case-based discussion, simulation, collaborative learning, and clinical problem solving.
Beyond educational theory, active learning is also supported by principles of cognitive neuroscience. Activities that require learners to retrieve, apply, discuss, and analyze information promote stronger memory consolidation and long-term retention through repeated activation of neural pathways. Furthermore, active learning engages higher-order cognitive processes associated with the prefrontal cortex, including critical thinking, decision making, cognitive flexibility, and clinical judgment. For nurse anesthesia students, whose future practice requires rapid synthesis of information and adaptation to dynamic patient conditions, educational approaches that emphasize active engagement may more closely mirror the cognitive demands encountered in clinical practice. Consequently, both adult learning theory and cognitive neuroscience provide support for FC strategies that prioritize application, discussion, and clinical reasoning over passive content delivery.
The second core theme compared was the student engagement levels. Several studies revealed an increase in learner engagement, motivation, and preferences for FC compared to traditional methods.9,16,17 This engagement was enhanced by collaborative group work, real-time response quizzes, and interactive technologies such as audience response systems and apps.4,8,18 Audience response systems allow for immediate feedback from participants or the audience to quickly gather data and enhance engagement. While these tools and strategies can significantly enhance student involvement, it is important to acknowledge that engagement barriers include variability in learner preparation and increased demand for pre-class work.8,9
Academic performance represents the third core theme, with multiple studies evaluating the impact of flipped learning on student outcomes. While findings are mixed, most research indicates generally positive effects on knowledge retention, critical thinking, and the application of course material in clinical contexts.9,19 This is further affirmed in meta-analysis favoring FC over traditional methods in health professions education.7,8,20 However, some studies report no significant difference in academic performance when comparing flipped learning to other active learning strategies such as simulation,1 highlighting the need for more rigorous, long-term assessments to determine its distinct impact on knowledge retention and clinical decision-making.21,22
The success of flipped learning is often tied to the seamless integration of educational technology, which supports both content delivery and in-class interactivity. This fourth core theme includes utilization of digital tools such as video lectures, learning management systems (e.g., Blackboard), mobile apps, and real-time response software to facilitate learning.4,8,23 It is widely accepted that technology is essential for scalability and accommodating adult learner’s schedules. Additionally, it supports personalized learning, feedback and enhanced interaction during both pre-class and in-class phases.12,24 Despite these advantages, the literature also highlights several challenges associated with technology integration that may limit its effectiveness if not intentionally addressed. These challenges include faculty familiarity with technology, resource availability,23,24 resistance to change, and limited collaboration among educators that may hinder widespread adoption.21
Building on the previous themes, the final core theme centers on the practical implementation barriers and facilitators that shape how successfully FCs are integrated into curricula. Common barriers included student non-compliance with pre-class preparation, faculty resistance or lack of training, and increased workload for educators.9,21 Some learners expressed dissatisfaction with certain in-class activities (e.g., reflective writing and group work) perceived as less engaging busy work and pre-class preparation as time-consuming.18,22 Reflective writing received the lowest satisfaction ratings, with some students perceiving greater benefit to faculty assessment than to their own learning. Several suggested reducing the frequency from weekly to every third week. Group work received the second lowest ratings, largely due to concerns that less-prepared students relied on peers to complete the work. Despite these limitations, facilitators included clear communication of expectations, faculty development programs, and use of engaging, high-quality pre-class material.25,26 The critical pieces included adequate technology infrastructure and student and teacher readiness for implementation to succeed.24
Theoretical Implications
Findings from the synthesis reinforce the theoretical premise that FC strategies are grounded in active learning theory, which prioritizes learner-centered instruction to cultivate higher-order cognitive skills, including critical thinking and problem solving.14,15,27 When compared to passive-lecture based methods, evidence suggest that FC enhances knowledge retention more effectively, indicating that active engagement with complex concepts of anesthesia is critical for long-term learning in graduate anesthesia education.9,22 Additionally, emerging theories on digital pedagogy and self-regulated learning highlight the role of technology in enabling autonomous learning through a wide range of platforms and tools, thereby enhancing the overall effectiveness of FC models.
When considering the outcomes of FC implementation, it is important to recognize the complexity of educational interventions, which are influenced by factors such as learner preparedness, faculty skills, and curriculum design.25,28 Given the variability in these outcomes, further research is needed to better understand how specific implementation barriers influence the effectiveness of FC models. Moreover, student-reported outcomes and perceptions of the FC model reinforce the importance of autonomy, flexibility, and relevance as key factors that drive motivation and engagement in adult learners.8,17,26
Practical Implications
Graduate nurse anesthesia programs are encouraged to adopt FC strategies to enhance learner engagement, improve knowledge retention, and align with evidence supporting active learning over traditional didactic methods.7,9,20 Successful implementation requires faculty development focused on addressing barriers such as technological proficiency, facilitation techniques, and managing learner preparation.9,24,25 Institutions should invest in the necessary resources and training to support this pedagogical shift. Integrating technology platforms can enhance the FC experience by providing real-time interaction, personalized feedback, and improved pre-class preparation to increase student participation and learning outcomes.4,12
While FC improves theoretical understanding and student engagement, it should be complemented by hands-on training and simulation to ensure procedural competency, especially in skill-intensive fields like anesthesia.1 Curriculum designers should focus FC content on high-yield, challenging topics while balancing pre-class workload and aligning assessments with higher-order thinking objectives.4,9,29 Collectively, this integrated approach supports deeper learning, reinforces clinical reasoning, and ensures that FC strategies translate into safe and competent clinical performance. Building on this evidence, the following section reflects on the practical application of FC strategies within graduate nurse anesthesia education, emphasizing instructional design decisions, faculty preparation, and lessons learned during implementation.
Educational Approach and Implementation
This section presents a reflective overview of the author’s experience implementing FC strategies within a graduate nurse anesthesia program, with emphasis on pre-class preparation, in-class instructional strategies, technology integration, and faculty preparation. Rather than serving as a formal research methodology, this narrative describes how evidence-informed FC principles were operationalized to support learner engagement, promote higher-order clinical reasoning, and align instructional practices with the cognitive and procedural demands of anesthesia education. This work represents a literature review and reflective analysis of educational practices rather than human subject’s research. Student feedback referenced in this manuscript was obtained through routine course evaluation processes and is presented in aggregate form without identifiers; therefore, Institutional Review Board review was not required. Collectively, the emphasized topics highlight practical considerations and lessons learned that may inform FC adoption across health sciences programs.
Pre-class Preparation
With student motivation and participation shown to correlate strongly with improved outcomes, FC design must consider how pre-class resources are developed and delivered to foster these qualities. To optimize student engagement and learning during the pre-class phase of the FC model, a deliberate effort was made to produce high quality, accessible video lectures that reflected the production standards students have come to expect from platforms such as YouTube. Recognizing that poor audio quality can hinder learning, a basic podcast microphone was used to ensure clear sound input while reducing background noise within recording software settings. This allowed students to increase playback volume without amplifying static or distortion, which improved clarity and comprehension of the content.
Lectures were recorded using OBS Studio, a free, open-source video recording and streaming platform with extensive customization features. OBS Studio allows users to input video from a personal webcam, audio from a microphone of choice, and live PowerPoint slide presentations. Multiple inputs can be overlaid to create dynamic recording scenes. For example, a webcam view of the instructor can be displayed alongside the PowerPoint content or removed entirely with a simple scene switch. The platform also supports input of YouTube videos, screen sharing from the instructor’s device, and smart tablet integration for drawing illustrations in real time. Each of these inputs can be organized into custom scenes that can be switched with a single click during recording.
OBS Studio includes settings for adjusting video output format and quality, as well as audio filters for noise suppression. It also features a pause-and-resume recording function that allows users to eliminate filler speech or errors without restarting the entire recording. This pause feature supports smooth transitions between scenes, reducing unnecessary footage and improving the efficiency of post-production editing.
Often, lecture content was recorded over the span of 2-3 days in smaller segments. These individual video files were then imported into Adobe Premiere Pro, a professional video editing platform, and compiled into a single, continuous lecture. Adobe Premiere’s intuitive timeline interface made it possible to arrange, trim, and merge multiple segments seamlessly. Its additional features allowed for cutting out errors, replacing slide visuals by dragging images directly into the timeline, adjusting audio gain, muting background noise, speeding up the video, and rearranging segments to improve flow and clarity. The ability to layer audio and video tracks, insert transitions, and make real-time adjustments to both sound and visuals gave greater control over the final product, even with basic editing knowledge acquired through publicly available tutorials.
To facilitate efficient post-production editing, the author intentionally continued recording for approximately 15 to 20 seconds after an error was made, rather than pausing immediately. This approach created a visible gap in the audio waveform, serving as a reliable marker for locating and trimming erroneous segments during the editing process. This made it easy to locate errors or segments requiring trimming without needing to listen through the entire recording. For post-recording editing, the Razor Tool in Adobe Premiere Pro allows precise trimming and seamless reconnection of clips, enabling lectures to continue smoothly without drawing attention to mistakes or requiring any explanation for student viewers.
Once editing was complete, the video was exported in a suitable format and uploaded privately to a dedicated YouTube channel. This approach offered secure cloud-based storage, link-based sharing, and easy access for students without requiring them to download large files. Students could watch the videos on any device, adjust playback speed, and review content at their own pace. Compared to traditional narrated PowerPoint recordings that required manual slide progression, this method offered a far more seamless and learner-centered experience. Ultimately, the goal was to provide high quality, thoughtfully produced lecture content well in advance of class sessions, allowing students to prepare effectively and ensuring that classroom time could be devoted to higher-order application and active learning strategies.
To support accessibility and accommodate diverse learning preferences, primary lecture notes were initially developed in Microsoft Word and then converted to PDF format for convenient file viewing across devices. For students who preferred a slide-based format, the same document was converted to PowerPoint using Adobe Acrobat’s “Convert to PowerPoint” feature. This version was also used by the instructor during video recording. Emphasis was placed on keeping slide content concise, with ample white space intentionally left below key points to allow students to create basic mind maps, insert relevant images, or add handwritten annotations. A typical course week posted in the Blackboard learning management system included a PDF of the lecture, a corresponding PowerPoint file, and a private YouTube link to the recorded video lecture. This multi-format approach to pre-class preparation aimed to provide students with flexible, organized, and high-quality resources to support individualized learning and readiness for in-class application.
In-Class Strategy
One of the greatest contributions a Certified Registered Nurse Anesthetist instructor can offer during in-person sessions is the sharing of clinical expertise and real-world application, which complements the content students have processed independently during pre-class preparation. When students arrive prepared, they are more likely to ask thoughtful, higher-level questions, allowing for deeper and more engaging discussion. This dynamic often leads to richer learning experiences that would be difficult to achieve in traditional, lecture-heavy formats. A particularly meaningful example occurred during a session on burn anesthesia, where students with prior intensive care unit experience caring for burn patients contributed valuable insights that elevated the depth and relevance of the conversation. Such contributions highlight the value of creating space for active dialogue and peer-to-peer learning, which may not be possible within the limitations of a traditional 1-2 hour lecture format.
To promote active learning, the primary classroom approach centered around structured case-based discussions. Many anesthesia textbooks include clinical cases, and there are also complete texts dedicated exclusively to themed case studies. In addition to curated resources, artificial intelligence tools such as ChatGPT were used to generate supplemental case scenarios tailored to specific course topics. These cases were often shared in advance, allowing students time to think critically about potential anesthetic plans, anticipate complications, and reflect on clinical decision-making before class. Classroom sessions also included interactive tools such as Kahoot, which created a fun and competitive environment while reinforcing key content through formative quizzing. Students often enjoyed selecting humorous usernames and competing for recognition, all while gaining exposure to the instructor’s question style and areas of emphasis.
On specific topic weeks, such as regional anesthesia or neuraxial techniques, class sessions were held in the simulation lab where equipment demonstrations and hands-on discussions enhanced comprehension and engagement. During these sessions, students were divided into small groups to facilitate peer-to-peer learning and collaborative exploration. For example, in the regional anesthesia lab, students used ultrasound equipment to identify relevant anatomical structures, building directly on prior lecture content from anatomy and pathophysiology. Working together, they located sonographic landmarks such as the brachial plexus, femoral nerve, or transverse abdominis plane and discussed how these structures relate to common block techniques. Faculty circulated among the groups to provide guidance and ask probing questions, but students led much of the discovery process themselves, reinforcing retention through experiential learning. This group-based approach not only strengthened procedural understanding but also promoted critical thinking, team communication, and confidence in using ultrasound as a clinical tool.
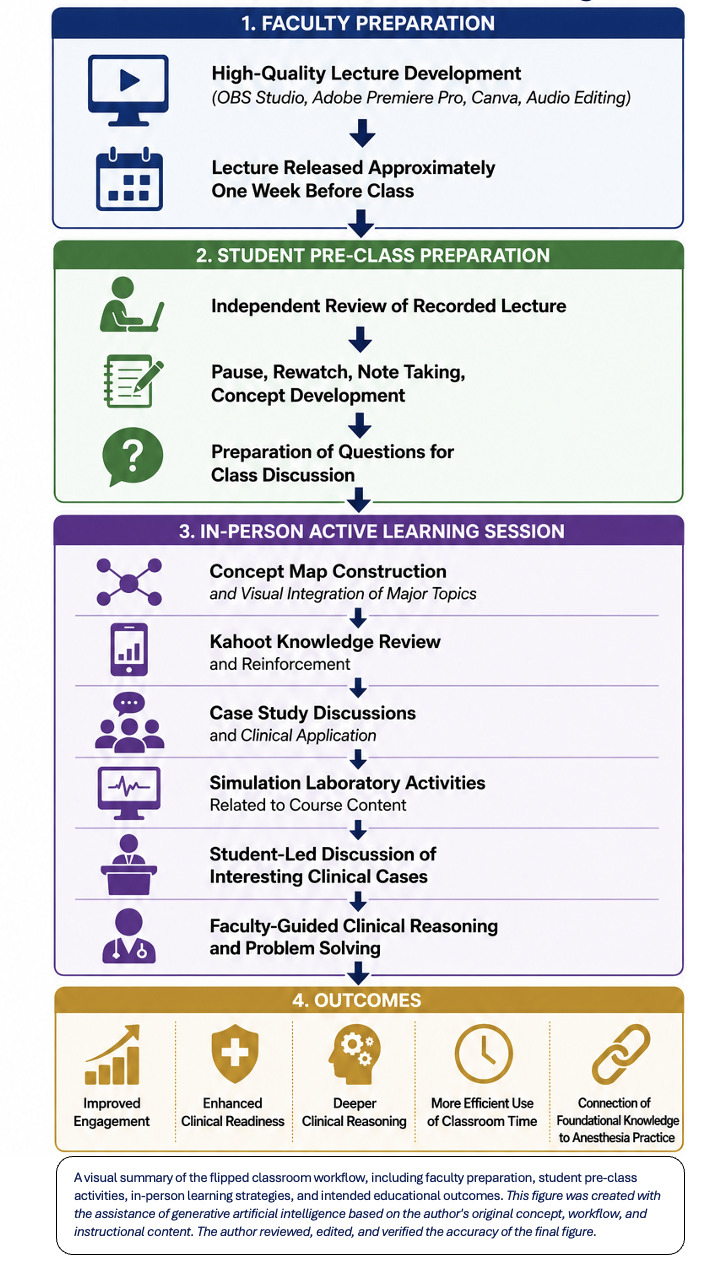
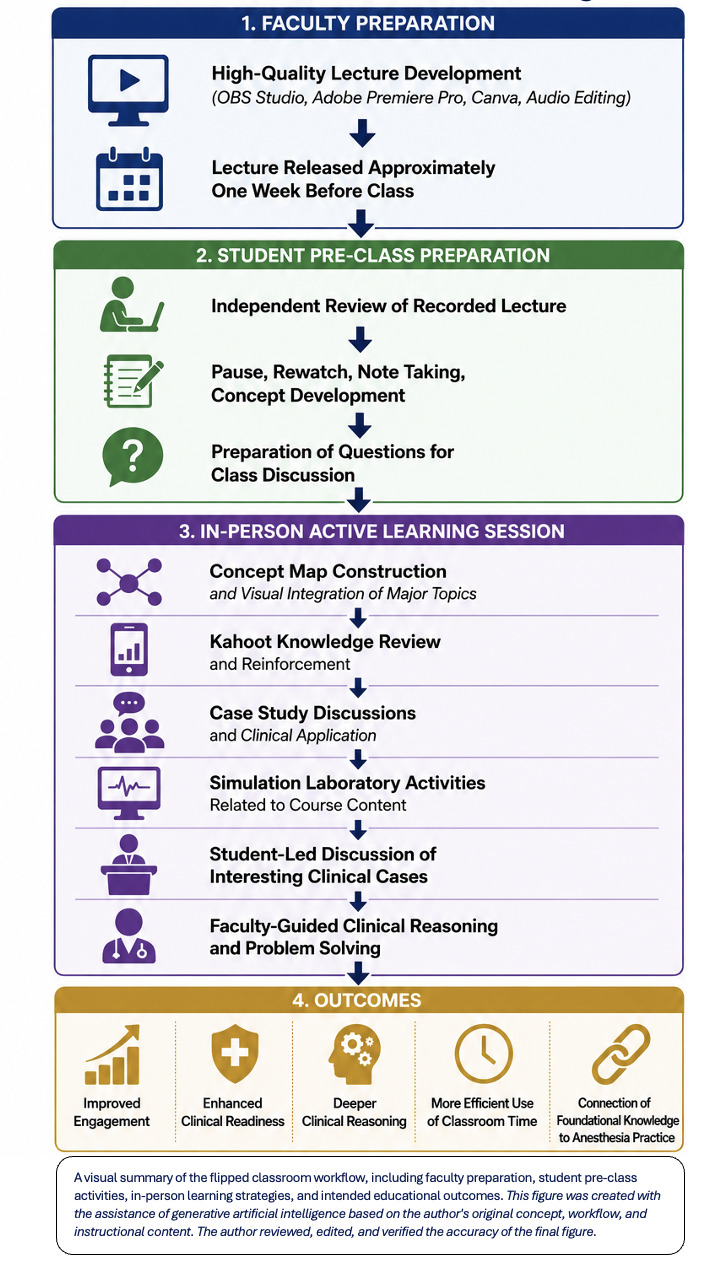
Another effective use of in-person time was dedicated to building clinical readiness before students were transitioning from shadowing experiences to a full-time clinical schedule. These sessions focused on the phases of anesthesia care in detail, including preoperative evaluation, intraoperative management, and postoperative considerations. Scenarios such as bronchospasm, laryngospasm, refractory hypotension, and difficult inductions were reviewed using practical, experience-based strategies. Faculty revisited foundational content taught earlier in the program, such as safe patient positioning, communication within the operating room, professional culture, and anesthesia delivery in non-operating room settings such as endoscopy suites. Classroom time was also used to explore miscellaneous topics such as ethical dilemmas or managing high-acuity patients, including an in-patient population with critical status who require anesthesia at the end of the clinical day with minimal backup. This comprehensive and interactive in-class strategy emphasized depth, clinical relevance, and collaboration, equipping students to transition more confidently into their roles as anesthesia providers. Figure 1 provides a visual overview of the FC workflow, highlighting faculty preparation, student-directed pre-class learning, active classroom engagement, and intended educational outcomes.
Artificial Intelligence Integration
In preparation for in-person learning and to enhance student readiness for active classroom engagement, the author acknowledged the importance of staying current with emerging artificial intelligence (AI) tools and platforms. Intentional efforts were made to explore and integrate AI-supported platforms that could enhance efficiency, content development, and learner engagement. Tools such as NotebookLM were utilized to support instructional design by summarizing large PDF documents, generating structured case studies, and creating podcast-style audio summaries from course materials to supplement student learning. Google AI Studio was also explored as a platform to assist with building simulation scenarios and supporting interactive educational content. Beyond individual tool use, participation in institutional AI initiatives and faculty committees was prioritized to better understand ethical considerations, best practices, and scalable applications of AI within higher education. Collectively, these approaches allowed faculty to reduce time spent on repetitive content development while increasing opportunities for higher-level learning activities, ultimately supporting improved student preparedness, deeper clinical reasoning, and more efficient use of instructional time.
Technology Integration
Implementing a FC model at this level of quality and functionality required a computer equipped with sufficient processing power, memory, and storage to handle resource-intensive tasks, such as video recording and editing with software like Adobe Premiere Pro, for example. A computer with upgraded hardware specifications helped prevent system lag, application crashes, and low-memory errors. To achieve high audio quality, the author used the RODE PodMic dynamic microphone, connected to a laptop through a Focusrite Scarlett USB Audio Interface Solo. For in-person class recordings and special events, such as the regional anesthesia seminar, a wireless microphone system (RODE Wireless Pro 2 Clip-On) was used to capture clear sound for playback.
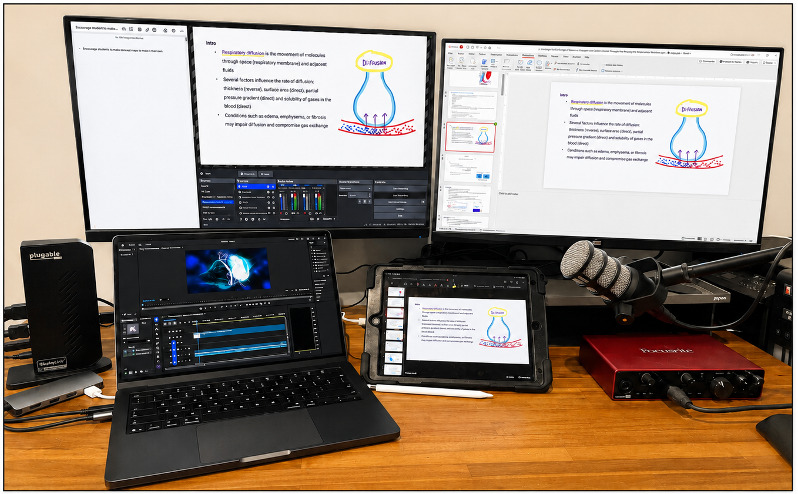
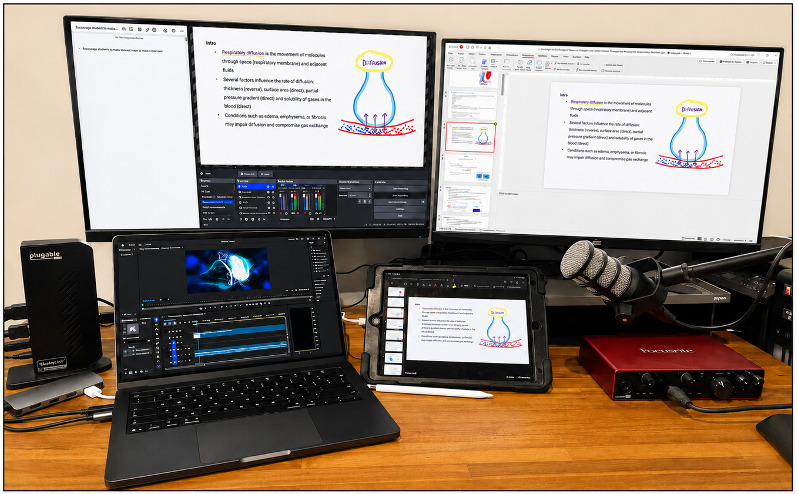
To support multitasking during lecture recordings, 2 additional monitors were connected to the laptop, enabling the simultaneous display of OBS Studio, PowerPoint slides, and teacher notes or online textbooks for reference. Recommendations for screen resolution and compatible hardware were obtained from a local computer specialist. For a Mac-based setup, an economical solution was identified using the Pluggable Dual DisplayPort and HDMI Docking Station from DisplayLink, which allowed for dual extended screens (Figure 2).
When a smartphone was used as a video recording device, a dedicated stand was used for stability. A multi-port dongle was often required to support simultaneous connections, including extended monitors, an audio interface, and a tablet input for drawing live illustrations. A Butterfly ultrasound probe was connected via the dongle for live demonstration recordings. Anatomy apps were also occasionally displayed in real time during recordings using this method. On one occasion, a live regional anesthesia workshop was recorded using an HDMI capture card, allowing input directly from an ultrasound machine into the laptop. This allowed the live scanning to be embedded as a scene in OBS Studio alongside the PowerPoint presentation, with the ability to switch between or simultaneously display the presenter’s probe manipulation via separate video input (e.g., smart phone camera).
Managing storage capacity was another essential consideration. Large video files were stored locally during editing, then uploaded to a secure cloud platform through YouTube. After confirming upload success, the local files were deleted to preserve computer storage. These YouTube videos could be re-downloaded at any time for future editing or reuse. Additional hardware included a podcast microphone stand, a dual monitor desk riser to elevate external screens, power surge protector, and an optional direct-wired ethernet connection to ensure stable internet during recording and uploading.
A variety of software tools also supported the production process. The Canva.com platform was used to create visually engaging presentation templates and short video introductions. Full video download capabilities required a subscription. EpidemicSound.com provided royalty-free background music for video introductions under a monthly licensing plan. Audio settings and device management were handled through the Focusrite Control application and RODE Central software, the latter of which was also used to retrieve backup recordings from the wireless microphone system. Together, these hardware and software components formed a robust infrastructure that supported the creation of high-quality, accessible lecture content for FC delivery.
Setting Clear Expectations
For a smooth transition into the FC model and to encourage student buy-in, accountability measures were intentionally kept informal during the initial phase, and no graded quizzes were assigned. The early emphasis was placed on building trust and fostering intrinsic motivation for pre-class preparation. This approach proved effective, as the strong momentum generated by student motivation and overwhelmingly positive feedback served as a primary driver for consistent engagement with assigned materials. Clearly communicating workload expectations and the purpose of independent learning activities early in the course was essential to the success of active learning strategies. To further promote engagement, test-style questions were strategically embedded at checkpoints within PowerPoint slides, and case studies were incorporated with instructor guidance for students to review in advance of class. When topics aligned with hands-on experiences in the simulation lab, such as neuraxial procedures, point of care ultrasound, or regional techniques, students were strongly encouraged to review related material beforehand to maximize participation in applied learning activities.
During in-person activities, including structured case discussions and interactive quiz platforms like Kahoot, it became evident that most students were arriving well prepared. Their readiness contributed to richer participation, deeper clinical reasoning, and more meaningful peer-to-peer learning. However, as the course progressed, it was recognized that maintaining consistent preparation across all learners required more structured accountability. To support this in planning for next cohort, the author plans to introduce brief online quizzes and readiness assessments before class sessions. These low-stakes evaluations serve to reinforce key concepts from the pre-class material while also signaling the importance of preparation as an expectation rather than a suggestion. This shift from informal to formal accountability helps to ensure that all students are equally engaged in the FC model and provide the faculty with timely feedback to address learning gaps and adapt instruction accordingly.
Discussion
Following 2 years of gradually integrating the FC model, a qualitative reflection was conducted to assess student engagement, classroom efficiency, student satisfaction, and faculty experience. One clear example of increased student engagement emerged during in-person sessions, where students frequently saved their questions from independent study time to ask the instructor during class. These questions often sparked broader discussions and deeper level of engagement, with peers contributing their own insights or attempting to answer their fellow students based on their understanding. These moments commonly led to additional follow-up questions from other students, transforming the classroom into a dynamic environment where multiple learners actively participated. This collaborative problem-solving and peer-to-peer interaction reflected critical thinking and demonstrated the effectiveness of the FC approach in promoting higher-order learning.
Students frequently expressed appreciation for the efficiency and flexibility offered by the FC model. Key benefits included consistency in lecture delivery, the ability to pause and resume recordings at their own pace, early development of concept maps, and the use of playback features such as YouTube’s speed adjustment function. More importantly, the model allowed for more effective use of limited instructional hours by reserving in-person time for higher-level learning and application-based discussions with expert clinicians. When time remained following these discussions, it was often used for hands-on learning in the simulation lab, one-on-one follow-up questions with the instructor, or timely topic reviews that aligned with students’ evolving needs. For example, clinical readiness discussions were held in response to rising student anxiety about the transition into clinical practice. By reducing prolonged lecture-based sessions into manageable and interactive learning blocks, the FC model supported a more engaging, student-centered environment that emphasized active learning and individualized support.
Student satisfaction outcomes were overwhelmingly positive, as reflected in qualitative feedback (see Appendix 1). Students consistently demonstrated a preference for this student-centered learning approach, frequently highlighting its flexibility, engagement, and relevance to clinical practice. The following are selected comments that illustrate recurring themes found throughout the broader set of responses provided: “I like the online lectures and in-person discussion/hands on skills. I feel like it’s more efficient and makes my life more flexible for me as a student to learn the material at home and come into class to apply it to real life scenarios.”; “…The effort and time he put into his lectures is greatly appreciated. I have found his use of the “reverse classroom” approach to be very helpful to allow myself to learn and digest the material before in-person classes. Reviewing the material prior to class allows me to apply the concepts to real-world practices and have meaningful discussions.” Many students expressed enthusiasm and appreciation for the FC model, citing its flexibility, the ability to absorb material at their own pace rather than cramming during extended in-person lectures, and the opportunity to revisit challenging concepts. They valued the increased potential for deeper-level follow-up discussions, expanded learning opportunities, and the freedom to devote additional time and focus to more difficult or high-priority topics.
A reflection on the faculty experience underscores the significant time investment required for the initial development of the FC model. Success hinged on thoughtful planning, early adoption of technology, and a sustained commitment to tasks such as lecture recording and preparation of pre-class case study activities, all of which were developed through a gradual and phased implementation of the FC model. Over time, the author continued to grow in the ability to design and tailor in-person sessions to maximize engagement and learning. This included the development of original case studies, formative quizzes, collaborative group activities, educational games, simulation sessions, high-priority topic reviews, and supplemental discussions that bridged recorded content with clinical application. Positive program outcomes were also closely tied to early and consistent communication of expectations, which helped students gradually acclimate to the FC structure and optimize their learning experience.
Lessons Learned
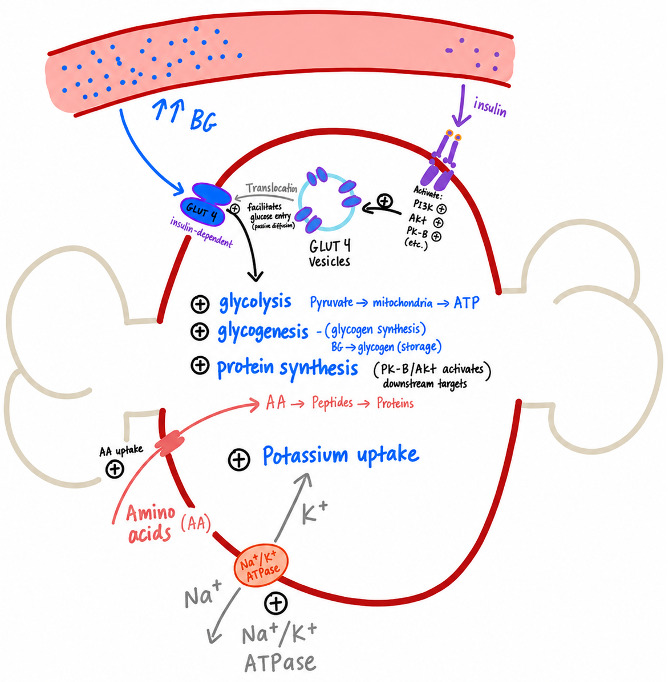
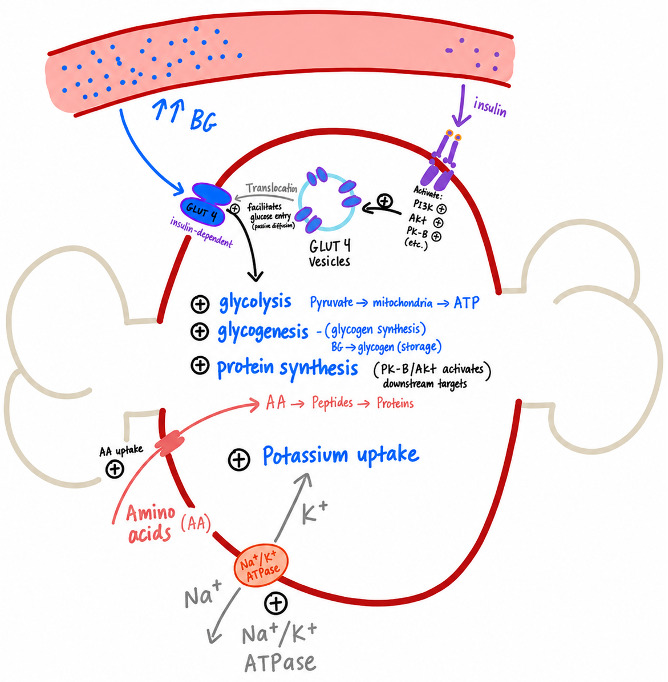
Implementing the FC model over a 2-year period yielded several practical lessons that informed its ongoing refinement. The observations described below reflect the author’s implementation experience and are intended to provide practical guidance for educators considering similar approaches. One of the earliest observations was that not all students arrived equally prepared for class in a self-directed learning environment. To support the success of the FC model, structured accountability measures should be incorporated through strategies such as short readiness quizzes or other pre-class preparation checks. During implementation, an informal accountability strategy included awarding bonus points to the top-performing students during Kahoot review activities, creating an incentive for learners to engage with lecture material before class. These tools may encourage consistent engagement with assigned content while providing faculty with valuable insight into student comprehension before class. Another important lesson was the shift in the faculty role from primarily delivering content to facilitating deeper discussion and application. This required instructors to arrive equally prepared with focused in-class materials, including case studies, supplemental slides featuring labeled images, fill-in-the-blank prompts, concept map drawings that summarized major topics into a single visual framework (Figure 3), and opportunities for collaborative note-taking and clinical reasoning.
One of the most consistent challenges was the lack of preparation among students on days with major exams in other courses. It became evident that exam days significantly reduced the time and energy students could devote to FC preparation. As a result, course scheduling must be designed with flexibility in mind, intentionally avoiding content heavy expectations during high stakes exam periods. Adjusting the course calendar to accommodate these patterns helped preserve student engagement and minimize cognitive overload.
From a technical perspective, several practical lessons emerged related to recording and editing video content. Conducting a short test recording before each session ensured that both audio and video were connected and functioning properly. When using a microphone setup, it was important to confirm that OBS Studio was recognizing the correct input source, with visible volume meter/bars confirming audio signal. Each recording scene within OBS Studio required a duplicate copy of the microphone settings to maintain consistent sound quality. Without this, transitions between scenes such as moving from a PowerPoint view to a tablet drawing screen overlay could default to the computer’s internal mic and result in a loss of quality.
Additionally, microphone filter settings needed to be tailored to the speaker’s distance from the microphone. Improper noise suppression could cause audio dropouts if the speaker moved too far from the microphone, leading to the need for re-recordings. Instructional YouTube tutorials proved helpful for optimizing OBS settings. To conserve storage space, video recordings were deleted only after being confirmed as fully functional on YouTube. If later editing was necessary, the recordings could be re-downloaded and revised using Adobe Premiere Pro.
Student feedback played a central role in refining FC practices, guiding adjustments to classroom structure and instructional activities. Each semester brought further growth and refinement. With lecture content reviewed independently, the greatest value from classroom time consistently came from activities that promoted clinical readiness, collaborative case-based problem solving, and focused exam preparation.
Conclusion
The FC model meaningfully enhances student engagement and improves the efficiency of instructional time, allowing learners to absorb foundational material independently and arrive to class prepared for deeper exploration. When thoughtfully designed and supported by faculty preparation, this approach proves to be both sustainable and impactful, particularly in nurse anesthesia programs where critical thinking and clinical application are essential. By shifting the focus from passive reception to active participation, the FC model supports the development of clinical-based practitioners who are better prepared for the complexities of anesthesia practice. It fosters habits of problem-solving and deep thinking that align directly with the demands of the profession, offering a clear path toward learner-centered, discussion-rich, and clinically relevant teaching. While the implementation experiences described in this manuscript are based on a narrative reflection from a single graduate nurse anesthesia program and may not be generalizable to all educational settings, they provide practical insights into the opportunities and challenges associated with adopting a FC model. Future research incorporating objective outcome measures, formal accountability strategies, and multi-institutional implementation may further clarify the impact of FC approaches in nurse anesthesia education.